Objective ·To evaluate the relationships between disc-condyle distance and anterior disc displacement, as well as between disc-condyle distance and disc morphology, in patients with temporomandibular disorders (TMD) using magnetic resonance imaging (MRI) of the temporomandibular joint (TMJ). Methods ·From September 2023 to March 2024, 90 patients (180 TMJs) who visited the TMJ clinic of Department of Stomatology, The Second Affiliated Hospital of Anhui Medical University, with clinical symptoms of TMD and were diagnosed via MRI with either anterior disc displacement or no significant displacement, were included. Clinical data were collected, and MRI images were used to measure the angle of disc displacement, disc-condyle distance, disc length, and thickness. The degree of disc deformation was assessed. The relationships between clinical symptoms and anterior disc displacement, between anterior disc displacement and both disc morphology and disc-condyle distance, and between disc-condyle distance and disc morphology were analyzed. Results ·Among the 90 patients, there were 16 males and 74 females, with a mean age of (28.1±14.5) years. Among the 180 TMJs, 175 had clinical symptoms and 5 were asymptomatic. There were 40 joints with no displacement, 78 with reducible anterior disc displacement, and 62 with irreducible anterior disc displacement. In the joints with irreducible anterior disc displacement, the proportion of those with two or more symptoms was slightly higher at 62.9%, but the difference was not statistically significant compared with the joints with no displacement or reducible anterior disc displacement. MRI assessment revealed that in the joints with irreducible anterior disc displacement, the proportion of disc deformation type Ⅲ or higher was significantly higher compared with the non-displaced joints (P<0.001). The disc length was significantly shorter (P<0.001), and the intermediate zone thickness was significantly greater (P<0.001) compared with the non-displaced joints. The disc displacement angles at centric closure and maximum opening were also significantly larger (P<0.001). The disc-condyle distance was 3.10 (2.70, 3.70) mm for non-displaced joints, 3.40 (3.00, 4.00) mm for joints with reducible anterior disc displacement, and 6.60 (4.78, 7.90) mm for joints with irreducible anterior disc displacement, with significant differences (P<0.001). The disc-condyle distance was 3.10 (2.80, 3.60) mm for type Ⅰ discs, 3.70 (3.10, 4.60) mm for type Ⅱ discs, 5.10 (4.00, 7.30) mm for type Ⅲ discs, and 6.80 (4.98, 8.20) mm for type Ⅳ/Ⅴ discs, with significant differences (P<0.001). The disc-condyle distance was negatively correlated with disc length (rs=-0.469, P<0.001), positively correlated with intermediate zone thickness (rs=0.319, P<0.001), and positively correlated with disc displacement angle at centric closure (rs=0.626, P<0.001). Conclusion ·With increasing severity of disc deformation, intermediate zone thickness, and disc displacement angle at centric closure, as well as decreasing disc length, the disc-condyle distance increases. The disc-condyle distance is an important indicator for MRI assessment of pathological changes in TMD.
SUN Lei, DAI Shifeng, CHEN Yuhua, XU Xinyi, JIANG Kele, LI Xiaowen, LI Chengjing, WU Tingting. Quantitative analysis of the distance between articular disc and condyle in patients with temporomandibular disorders. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2025, 45(6): 684-692 doi:10.3969/j.issn.1674-8115.2025.06.003
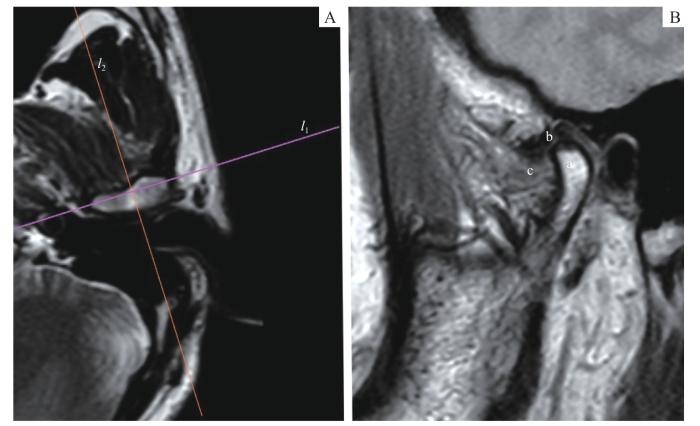
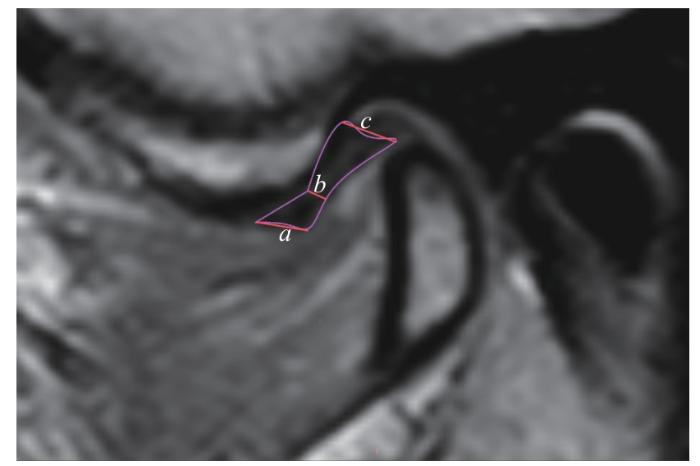
Note: PDWI images. A. Axial plane. l1—the transverse axis of the condyle (the line connecting the internal and the external poles of the condyle); l2—the positioning plane perpendicular to the condylar transverse axis. B. Oblique sagittal plane. a—condyle; b—articular disc; c—lateral pterygoid muscle.
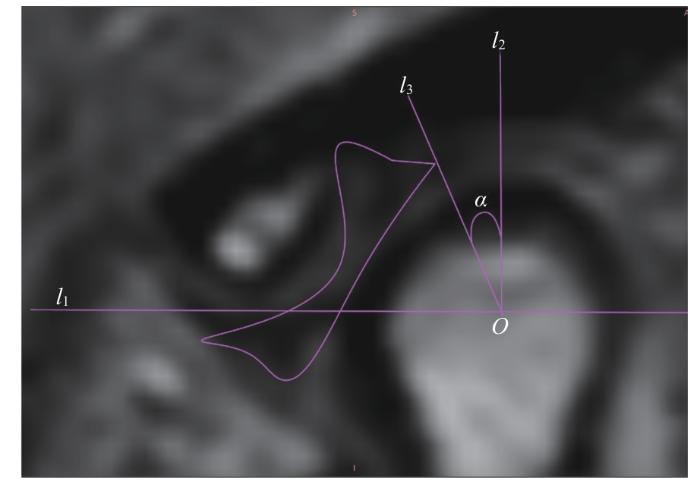
Note: An oblique sagittal PDWI image. l1—the line connecting the articular eminence and the vertex of the posterior tubercle; O—the midpoint of the intersection of line l1 with the condyle; l2—the perpendicular line to l1 through point O; l3—the line connecting the posterior edge of the articular disc with point O; α—the angle between l2 and l3, which is the angle of disc displacement.
Fig 3
Measurement of articular disc displacement angle
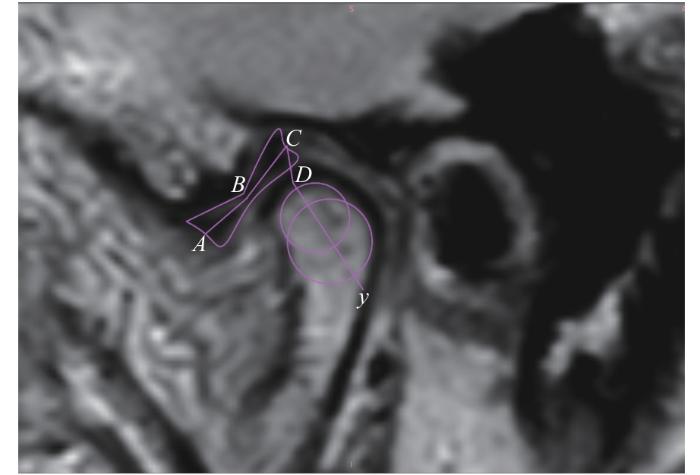
Note: An oblique sagittal PDWI image. A—the midpoint of the anterior edge of the anterior band of the articular disc; B—the midpoint of the intermediate zone of the articular disc; C—the midpoint of the posterior edge of the posterior band of the articular disc; y—the long axis of the condylar head; D—the intersection of y-axis with the condyle; AB+BC—the length of the articular disc; CD—the disc-condyle distance.
Fig 4
Measurement of disc-condyle distance and articular disc length
The study has been reviewed and approved by the Ethics Committee of Hospital of Stomatology, Anhui Medical University (Approval No. HM2024001). The study was a retrospective study, and informed consent was exempted.
HAN Longchuan was primarily responsible for conducting experiments, organizing and analyzing data, and drafting and revising the manuscript. LI Yue contributed to experimental operations and manuscript revision. ZOU Zhihui and LUO Jing participated in data analysis and manuscript revisions. LI Ruoyi contributed to animal experiments and manuscript revisions. ZHANG Yingting, TANG Xinxin, TIAN Lihong, LU Yuheng and HUANG Ying participated in manuscript revisions. HE Ming and FU Yinkun were responsible for project design and manuscript revisions. All authors have read the final version of the paper and agreed to its submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
AIELLO V, FERRILLO M, MAROTTA N, et al. Temporomandibular joint arthritis in rheumatic diseases patients: which are the effective rehabilitative approaches for pain relief? A systematic review[J]. BMC Musculoskelet Disord, 2025, 26(1): 159.
BADRI O, DAVIS C M, WARBURTON G. Arthroscopic management and recent advancements in the treatment of temporomandibular joint disorders[J]. Br J Oral Maxillofac Surg, 2024, 62(9): 820-825.
WARZOCHA J, GADOMSKA-KRASNY J, MROWIEC J. Etiologic factors of temporomandibular disorders: a systematic review of literature containing diagnostic criteria for temporomandibular disorders (DC/TMD) and research diagnostic criteria for temporomandibular disorders (RDC/TMD) from 2018 to 2022[J]. Healthcare (Basel), 2024, 12(5): 575.
BERNKOPF E, NARDONE M, CAPRIOTTI V. Follow-up clarifications concerning the authors' reply to the 'look at the elephant!' comment on 'prevalence of temporomandibular disorders in adult obstructive sleep apnoea patients: a cross-sectional controlled study'[J]. J Oral Rehabil, 2024, 51(10): 2234-2236.
DWORKIN S F, LERESCHE L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique[J]. J Craniomandib Disord, 1992, 6(4): 301-355.
SCHIFFMAN E, OHRBACH R, TRUELOVE E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group[J]. J Oral Facial Pain Headache, 2014, 28(1): 6-27.
AZMA R, HAREENDRANATHAN A, LI M X, et al. Automated pediatric TMJ articular disk identification and displacement classification in MRI with machine learning[J]. J Dent, 2025, 155: 105622.
AKAI H, YASAKA K, SUGAWARA H, et al. Faster acquisition of magnetic resonance imaging sequences of the knee via deep learning reconstruction: a volunteer study[J]. Clin Radiol, 2024, 79(6): 453-459.
LI C J, ZHANG Q B. Comparison of magnetic resonance imaging findings in 880 temporomandibular disorder patients of different age groups: a retrospective study[J]. BMC Oral Health, 2022, 22(1): 651.
WOJCIECHOWSKA B, SZARMACH A, MICHCIK A, et al. Association between clinical manifestations in temporomandibular joint disorders and corresponding radiographic findings[J]. J Clin Med, 2024, 13(16): 4886.
ZHU J Y, GONG Y J, ZHENG F J, et al. Relationships between functional temporomandibular joint space and disc morphology, position, and condylar osseous condition in patients with temporomandibular disorder[J]. Clin Oral Investig, 2024, 28(3): 193.
CHEN B Y, LI C J. The relationship between the articular disc in magnetic resonance imaging and the condyle in cone beam computed tomography: a retrospective study[J]. J Stomatol Oral Maxillofac Surg, 2024, 125(5S1): 101940.
ZHANG G L, LIAO Y Y, WU M N, et al. Study on MRI features of disc-condylar complex and semiquantitative evaluation of peridisc attachment in cases of temporomandibular joint disc displacement[J]. Chinese Journal of Magnetic Resonance Imaging, 2024, 15(2): 7-13.
KOCA C G, GÜMRÜKÇÜ Z. Does clinical findings correlate with magnetic resonance imaging (MRI) findings in patients with temporomandibular joint (TMJ) pain? A cross sectional study[J]. Med Oral Patol Oral Cir Bucal, 2020, 25(4): e495-e501.
ZHANG Y Y, YI J R, PAN C. Quantitative MR study of morphological changes in articular disc cartilage in patients with temporomandibular disorders[J]. Journal of Clinical Radiology, 2024, 43(11): 1865-1871.
ARAYASANTIPARB R, TSUCHIMOCHI M. Quantification of disc displacement in internal derangement of the temporomandibular joint using magnetic resonance imaging[J]. Odontology, 2010, 98(1): 73-81.
YANG Z J, WANG M G, MA Y W, et al. Magnetic resonance imaging (MRI) evaluation for anterior disc displacement of the temporomandibular joint[J]. Med Sci Monit, 2017, 23: 712-718.
XIE Q Y, YANG C, HE D M, et al. Will unilateral temporomandibular joint anterior disc displacement in teenagers lead to asymmetry of condyle and mandible? A longitudinal study[J]. J Craniomaxillofac Surg, 2016, 44(5): 590-596.
ZHANG Q, YE Z, WU Y G, et al. Nonlinear relationship between temporomandibular joint disc displacement distance and disc length: a magnetic resonance imaging analysis[J]. J Clin Med, 2022, 11(23): 7160.
LI Z Y, ZHOU J L, YU L X, et al. Disc-condyle relationship alterations following stabilization splint therapy or arthrocentesis plus hyaluronic acid injection in patients with anterior disc displacement: a retrospective cohort study[J]. Oral Radiol, 2023, 39(1): 198-206.
FU K Y, HU M, YU Q, et al. Experts consensus on MRI examination specification and diagnostic criteria of temporomandibular joint disc displacement[J]. Chinese Journal of Stomatology, 2020, 55(9): 608-612.
DRACE J E, ENZMANN D R. Defining the normal temporomandibular joint: closed-, partially open-, and open-mouth MR imaging of asymptomatic subjects[J]. Radiology, 1990, 177(1): 67-71.
PERSCHBACHER S. Chapter 27: temporomandibular joint abnormalities[M]//WHITE S C, PHAROAH M J. Oral radiology: principles and interpretation. 7th ed. St. Louis: Mosby, 2013: 492-523.
INCESU L, TAŞKAYA-YILMAZ N, OĞÜTCEN-TOLLER M, et al. Relationship of condylar position to disc position and morphology[J]. Eur J Radiol, 2004, 51(3): 269-273.
WANG M Q, CAO H T, GE Y L, et al. Magnetic resonance imaging on TMJ disc thickness in TMD patients: a pilot study[J]. J Prosthet Dent, 2009, 102(2): 89-93.
HU Y K, YANG C, XIE Q Y. Changes in disc status in the reducing and nonreducing anterior disc displacement of temporomandibular joint: a longitudinal retrospective study[J]. Sci Rep, 2016, 6: 34253.
MAIZLIN Z V, NUTIU N, DENT P B, et al. Displacement of the temporomandibular joint disk: correlation between clinical findings and MRI characteristics[J]. J Can Dent Assoc, 2010, 76: a3.
LIU Z J, YAMAGATA K, KUROE K, et al. Morphological and positional assessments of TMJ components and lateral pterygoid muscle in relation to symptoms and occlusion of patients with temporomandibular disorders[J]. J Oral Rehabil, 2000, 27(10): 860-874.
TOGNINI F, MANFREDINI D, MONTAGNANI G, et al. Is clinical assessment valid for the diagnosis of temporomandibular joint disk displacement?[J]. Minerva Stomatol, 2004, 53(7/8): 439-448.
YAN S, QIAO Y M, DUAN L W. Analysis of clinical changes and magnetic resonance imaging features of 37 patients with temporomandibular joint disc condylar complex with anterior disc displacement without reduction[J]. West China Journal of Stomatology, 2024, 42(1): 82-88.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}