目的·以氯氮平-氟伏沙明合用为例,通过构建针对中国群体的生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型,预测氯氮平联合用药的药物相互作用(drug-drug interaction,DDI)并对氯氮平进行剂量优化。方法·通过文献及药理学相关数据库获取氯氮平及氟伏沙明的基本理化性质参数,药物吸收、分布、代谢及排泄(absorption,distribution, metabolism and excretion,ADME)相关参数及中国群体的生理解剖相关参数,利用PK-Sim®软件构建2种药物的PBPK模型。以平均百分比误差(mean percentage error,MPE)和平均绝对百分比误差(mean absolute percentage error,MAPE),或者预测药时曲线下面积(area under the curve,AUC)或峰浓度(peak concentration,Cmax)与实测AUC或Cmax的比值为判断指标,并通过真实世界血药浓度数据进行模型验证。在此基础上结合氟伏沙明对氯氮平的抑制作用参数构建氯氮平-氟伏沙明联合用药的PBPK模型,预测氯氮平的药物代谢动力学变化。以药时曲线下面积比值(area under the curve ratio,AUCR)或峰浓度比值(peak concentration ratio,CmaxR)的90%置信区间为评价指标判断是否存在临床显著的DDI(无效应边界为80%~125%)。根据PBPK模型量化氯氮平-氟伏沙明联合用药后氯氮平的药物代谢动力学变化,并制定氯氮平的剂量优化方案。结果·构建的氯氮平、氟伏沙明模型验证的MPE绝对值≤10%且MAPE<25%,说明预测的药时曲线是准确的。氯氮平-氟伏沙明合用的PBPK模型的AUC预测值与实测值的比值在1.25以内,可准确地预测药物代谢动力学参数。氯氮平-氟伏沙明联用模型的预测结果提示,氯氮平-氟伏沙明联合用药的AUCR和CmaxR的90%置信区间均不完全位于无效应边界内,说明两药合用会发生临床显著性的DDI。此外,PBPK模型的剂量优化结果提示:受试者联合服用氯氮平及氟伏沙明时,氯氮平的剂量减少至原本剂量的50%,可使氯氮平的暴露水平与单药治疗时保持一致。结论·研究建立的PBPK模型可以较好模拟联合用药对氯氮平药物代谢动力学的影响,对于预测药物可能的相互作用及剂量优化方案有参考意义。如果治疗过程中需要合用氯氮平和氟伏沙明,须警惕临床显著的DDI,并应优化氯氮平的剂量。
关键词:氯氮平
;
联合用药
;
药物相互作用
;
生理药物代谢动力学模型
Abstract
Objective ·To develop physiologically based pharmacokinetic (PBPK) models specifically designed for the Chinese population by utilizing the combination of clozapine and fluvoxamine as a case, and predict the drug-drug interaction (DDI) associated with the combination medication of clozapine, ultimately optimizing the dosage of clozapine. Methods ·By obtaining the physicochemical parameters, absorption, distribution, metabolism, excretion (ADME)-related parameters, and physiologically relevant parameters of the Chinese population through literature and pharmacology-related databases, PBPK models for the clozapine and fluvoxamine were constructed by using PK-Sim® software. The models′ accuracy was evaluated by comparing predicted values of the area under the curve (AUC) and peak concentration (Cmax) to observed data, using the mean percentage error (MPE) and mean absolute percentage error (MAPE) as evaluation indicators. The models were validated against real-world plasma drug concentration data. Additionally, combining the inhibitory effect of fluvoxamine on clozapine, models for the combination therapy of clozapine and fluvoxamine were developed to predict the pharmacokinetic changes of clozapine. The presence of clinically significant DDI was determined by using the 90% confidence interval of the AUC ratio (AUCR) or Cmax ratio (CmaxR) as evaluation metrics, with a non-effect boundary set at 80%‒125%. The pharmacokinetic changes of clozapine upon co-administration with fluvoxamine based on PBPK models were quantified, and a dosage optimization for clozapine was developed. Results ·The constructed model of clozapine and fluvoxamine was considered accurate if the absolute value of the MPE was ≤10% and the MAPE was <25% during validation, indicating that the predicted concentration-time curves were accurate. The PBPK model for the co-administration of clozapine and fluvoxamine was able to accurately predict pharmacokinetic parameters if the ratio of predicted AUC to observed AUC was within 1.25. The prediction of PBPK model for the co-administration showed that the 90% confidence intervals for AUCR and CmaxR of the combination therapy of clozapine and fluvoxamine were not entirely within the ineffective effect boundary, indicating a clinically significant DDI when these two drugs were used concomitantly. Moreover, the dose optimization according to the PBPK models indicated that when subjects were co-administered with clozapine and fluvoxamine, reducing the dose of clozapine to 50% of the original dose could maintain the exposure levels of clozapine consistent with monotherapy. Conclusion ·The established PBPK model can effectively simulate the impact of combination therapy on pharmacokinetic changes of clozapine, providing valuable insights for predicting potential DDI and optimizing dosage regimens. If clozapine needs to be co-administered with fluvoxamine during the treatment, clinicians should remain vigilant for clinically significant DDI and contemplate optimizing the dosage of clozapine accordingly.
Keywords:clozapine
;
combination medication
;
drug-drug interaction
;
physiologically based pharmacokinetic model
MOU Fan, HUANG Zhiwei, CHENG Yu, ZHAO Xue, LI Huafang, YU Shunying. Prediction of drug-drug interactions in clozapine combination therapy based on physiologically based pharmacokinetic model. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(11): 1414-1421 doi:10.3969/j.issn.1674-8115.2024.11.008
氯氮平是难治性精神分裂症优先考虑的药物。氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2]。氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4]。美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7]。生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10]。若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]。
Note: Sample 1, Sample 2, and Sample 3 were from three clinical studies, each containing measurement data of CYP450 enzyme levels in the Chinese populations. CYP450—cytochrome P450; WM—weighted mean; “-” indicating missing data.
从相应的临床试验中获取年龄、性别、身高及体质量等人口学特征的信息以构建虚拟群体;若缺乏相关信息则从美国国家健康与营养调查(National Health and Nutrition Examination Survey,NHANES)数据库中获取。
(2)药物模块及给药方案模块。在药物数据库(DrugBank)等药理学数据库、FDA以及文献中收集药物的基本理化性质参数及药物吸收、分布、代谢及排泄(absorption,distribution,metabolism and excretion,ADME)相关参数来建立药物模块。经文献检索和各药理学数据库检索收集的氯氮平及氟伏沙明的基本理化性质参数与ADME相关参数详见表2。氯氮平的给药方案有2种,分别是:150 mg/次,2次/d;100 mg/次,2次/d。
Tab 2
表2
表2氯氮平和氟伏沙明的基本理化性质及ADME相关参数
Tab 2 Basic physicochemical properties and ADME-related parameters of clozapine and fluvoxamine
Parameter
Clozapine
Source
Fluvoxamine
Source
LogP
3.23
DrugBank
3.68
Fitted
fu
0.02
FDA, fitted
0.20
DrugBank, fitted
Molecular weight/(g·mol-1)
326.83
DrugBank
318.34
DrugBank
pKa
7.50
DrugBank
9.40
Fitted
Solubility/(mg·mL-1)
0.19
ALOGPS
0.07
Fitted
CLh/(mL·h-1·kg-1)
2.28
Fitted
1.21
Fitted
CLr/(mL·h-1·kg-1)
0.01
Fitted
0.02
FDA, fitted
Note: Fitted represents the parameters obtained from fitting the PBPK model. LogP—logarithm of octanol/water partition coefficient; fu—fraction unbound; pKa—negative decadic logarithm of acid dissociation constant; CLh—hepatic clearance; CLr—renal clearance.
(1)模型验证的评价指标。PBPK模型可以从2个方面进行验证。一是以平均百分比误差(mean percentage error,MPE)和平均绝对百分比误差(mean absolute percentage error,MAPE)为评价依据,当MPE绝对值≤10%且MAPE<25%时模型预测的药时曲线是准确的(公式3、4)[18]。二是以预测药时曲线下面积(area under the curve,AUC)或峰浓度(peak concentration,Cmax)与实测AUC或Cmax的比值为判断指标,当预测值与实测值的比值在1.25倍内可认为预测药物代谢动力学参数的准确度较高。
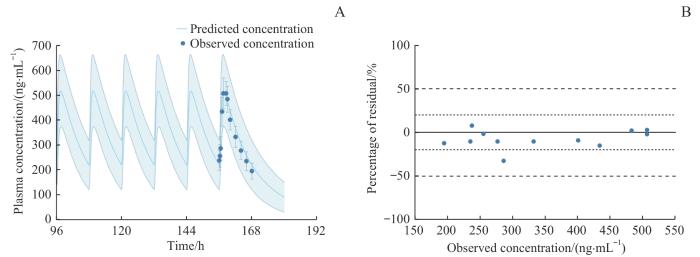
Note: A. Plasma concentration-time curve profiles of clozapine after the administration of multiple oral 100 mg tablets in healthy adults. B. Residue plot for the model prediction of clozapine plasma concentrations in healthy adults.
Fig 1
Plasma concentration-time curve profiles and residue plot of clozapine after multiple oral doses of 100 mg in healthy adults
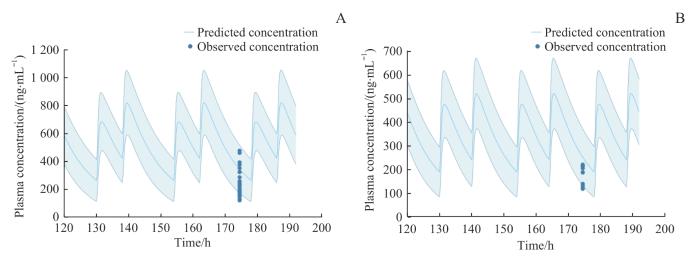
Note: A. Plasma concentration-time curve profiles of clozapine after the administration of multiple 150 mg oral tablets in patients. B. Plasma concentration-time curve profiles of clozapine after the administration of multiple 100 mg oral tablets in patients.
Fig 2
Plasma concentration-time curve profiles of clozapine after the administration of multiple oral tablets of clozapine in patients
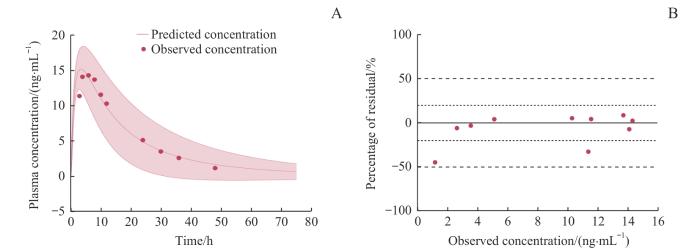
Note: A. Plasma concentration-time curve profiles of fluvoxamine after the administration of a single 50 mg dose of fluvoxamine in healthy adults. B. Residue plot for the model prediction of fluvoxamine plasma concentrations in healthy adults.
Fig 3
Plasma concentration-time curve profiles and residue plot of fluvoxamine after the administration of a single 50 mg dose of fluvoxamine in healthy adults
Tab 3 Comparison of pharmacokinetic parameters of clozapine-fluvoxamine PBPK model
Drug administration
Pharmacokinetic parameter
Combination therapy/monotherapy
No effect boundary
mean/%
90%CI
Administration 1
Cmax/(ng·mL-1)
180
111%‒223%
80%‒125%
AUC/(ng·h·mL-1)
197
105%‒204%
Administration 2
Cmax/(ng·mL-1)
175
110%‒240%
AUC/(ng·h·mL-1)
189
100%‒277%
Note: Administration 1 and 2 respectively involved subjects taking oral clozapine at either 100 mg or 150 mg twice daily, and 50 mg once daily. CI—confidence interval.
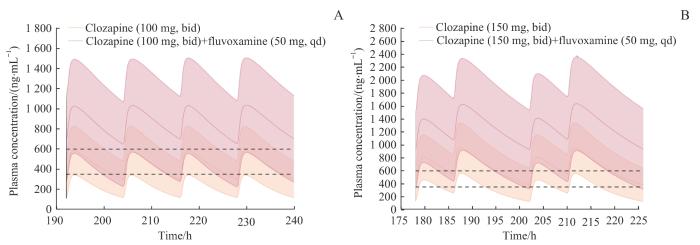
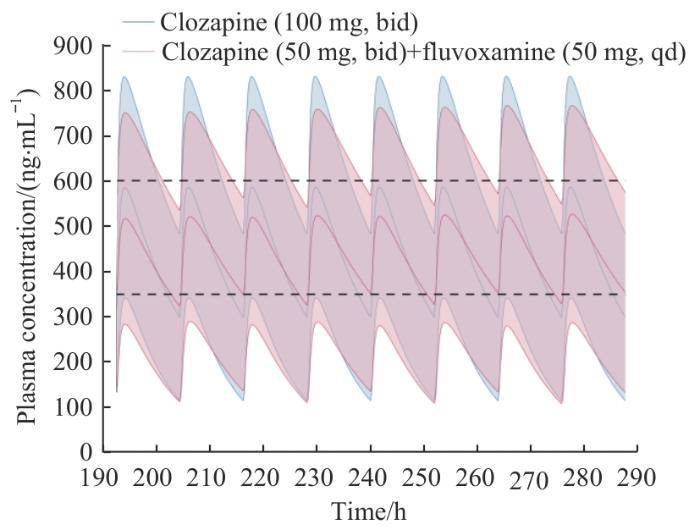
Note: A. Plasma concentration-time curve profiles of clozapine (100 mg) before and after combination with fluvoxamine (50 mg). B. Plasma concentration-time curve profiles of clozapine (150 mg) before and after combination with fluvoxamine (50 mg). bid—twice a day; qd—once a day.
Fig 4
Comparison of plasma concentration-time curve profiles of clozapine before and after combination with fluvoxamine
YU Shunying designed and supervised the entire research project; MOU Fan participated in research design, and completed data collection, model construction, validation, and paper writing; HUANG Zhiwei participated in guiding model construction and validation; CHENG Yu and ZHAO Xue participated in data collection and organization; HUANG Zhiwei, LI Huafang and YU Shunying participated in paper revisions. All the authors have read the last version of the manuscript and consented to submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclosed no relevant conflict of interests.
VERDOUX H, QUILES C, DE LEON J. Optimizing co-prescription of clozapine and antiseizure medications: a systematic review and expert recommendations for clinical practice[J]. Expert Opin Drug Metab Toxicol, 2024, 20(5): 347-358.
VERDOUX H, QUILES C, DE LEON J. Risks and benefits of clozapine and lithium co-prescribing: a systematic review and expert recommendations[J]. Schizophr Res, 2024, 268: 233-242.
AUGUSTIN M, SCHORETSANITIS G, PFEIFER P, et al. Effect of fluvoxamine augmentation and smoking on clozapine serum concentrations[J]. Schizophr Res, 2019, 210: 143-148.
RAFIZADEH R, SOOCH A, RISI A, et al. Impact of patient-specific factors on clozapine metabolism in individuals with treatment-resistant schizophrenia or schizoaffective disorder[J]. J Psychopharmacol, 2024, 38(6): 526-531.
DE LEON J, RAJKUMAR A P, KAITHI A R, et al. Do Asian patients require only half of the clozapine dose prescribed for caucasians? A critical overview[J]. Indian J Psychol Med, 2020, 42(1): 4-10.
HASSAB ERRASOUL A, ALARABI M A. Factors predicting serum clozapine levels in Middle Eastern patients: an observational study[J]. BMC Psychiatry, 2022, 22(1): 269.
CHO C K, KANG P, JANG C G, et al. PBPK modeling to predict the pharmacokinetics of venlafaxine and its active metabolite in different CYP2D6 genotypes and drug-drug interactions with clarithromycin and paroxetine[J]. Arch Pharm Res, 2024, 47(5): 481-504.
ZHANG Z C, HU M, XUAN D L, et al. Physiologically based pharmacokinetic (PBPK) modeling of BDE-209 following oral exposure in Chinese population[J]. Food Chem Toxicol, 2022, 169: 113416.
LIN W, CHEN Y, UNADKAT J D, et al. Applications, challenges, and outlook for PBPK modeling and simulation: a regulatory, industrial and academic perspective[J]. Pharm Res, 2022, 39(8): 1701-1731.
WILLCOCKS I R, LEGGE S E, NALMPANTI M, et al. Clozapine metabolism is associated with absolute neutrophil count in individuals with treatment-resistant schizophrenia[J]. Front Pharmacol, 2021, 12: 658734.
VAQUERO-BAEZ M, DÍAZ-RUÍZ A, TRISTÁN-LÓPEZ L, et al. Clozapine and desmethylclozapine: correlation with neutrophils and leucocytes counting in Mexican patients with schizophrenia[J]. BMC Psychiatry, 2019, 19(1): 295.
VERDOUX H, QUILES C, DE LEON J. Optimizing antidepressant and clozapine co-prescription in clinical practice: a systematic review and expert recommendations[J]. Schizophr Res, 2024, 268: 243-251.
ZHANG H F, WANG H H, GAO N, et al. Physiological content and intrinsic activities of 10 cytochrome P450 isoforms in human normal liver microsomes[J]. J Pharmacol Exp Ther, 2016, 358(1): 83-93.
SHU Y, CHENG Z N, LIU Z Q, et al. Interindividual variations in levels and activities of cytochrome P-450 in liver microsomes of Chinese subjects[J]. Acta Pharmacol Sin, 2001, 22(3): 283-288.
AN X X, YU Y C, LI G F, et al. Abundance and associated variations of cytochrome P450 drug-metabolizing enzymes in the liver of East Asian adults: a meta-analysis[J]. Eur J Drug Metab Pharmacokinet, 2021, 46(2): 225-233.
ZHU J Y, ZHOU S F, WANG L, et al. Characterization of pediatric rectal absorption, drug disposition, and sedation level for midazolam gel using physiologically based pharmacokinetic/pharmacodynamic modeling[J]. Mol Pharm, 2024, 21(5): 2187-2197.
OWEN J S, FIEDLER-KELLY J. Introduction to population pharmacokinetic/pharmcodynamic analysis with nonlinear mixed effects models[M]. Beijing: Chemical Industry Press, 2020: 69.
ORLANDO R, DE MARTIN S, ANDRIGHETTO L, et al. Fluvoxamine pharmacokinetics in healthy elderly subjects and elderly patients with chronic heart failure[J]. Br J Clin Pharmacol, 2010, 69(3): 279-286.
MALLIKAARJUN S, SALAZAR D E, BRAMER S L. Pharmacokinetics, tolerability, and safety of aripiprazole following multiple oral dosing in normal healthy volunteers[J]. J Clin Pharmacol, 2004, 44(2): 179-187.
FUKASAWA T, YASUI-FURUKORI N, SUZUKI A, et al. Effects of caffeine on the kinetics of fluvoxamine and its major metabolite in plasma after a single oral dose of the drug[J]. Ther Drug Monit, 2006, 28(3): 308-311.
LU M L, LANE H Y, CHEN K P, et al. Fluvoxamine reduces the clozapine dosage needed in refractory schizophrenic patients[J]. J Clin Psychiatry, 2000, 61(8): 594-599.
KARJALAINEN M J, NEUVONEN P J, BACKMAN J T. In vitro inhibition of CYP1A2 by model inhibitors, anti-inflammatory analgesics and female sex steroids: predictability of in vivo interactions[J]. Basic Clin Pharmacol Toxicol, 2008, 103(2): 157-165.
YAO C, KUNZE K L, KHARASCH E D, et al. Fluvoxamine-theophylline interaction: gap between in vitro and in vivo inhibition constants toward cytochrome P4501A2[J]. Clin Pharmacol Ther, 2001, 70(5): 415-424.
OLESEN O V, LINNET K. Fluvoxamine-clozapine drug interaction: inhibition in vitro of five cytochrome P450 isoforms involved in clozapine metabolism[J]. J Clin Psychopharmacol, 2000, 20(1): 35-42.
KIKUCHI R, CHOTHE P P, CHU X Y, et al. Utilization of OATP1B biomarker coproporphyrin-I to guide drug-drug interaction risk assessment: evaluation by the pharmaceutical industry[J]. Clin Pharmacol Ther, 2023, 114(6): 1170-1183.
SCHORETSANITIS G, KANE J M, CORRELL C U, et al. Blood levels to optimize antipsychotic treatment in clinical practice: a joint consensus statement of the American society of clinical psychopharmacology and the therapeutic drug monitoring task force of the arbeitsgemeinschaft für neuropsychopharmakologie und pharmakopsychiatrie[J]. J Clin Psychiatry, 2020, 81(3): 19cs13169.
BEREL C, MOSSÉ U, WILS J, et al. Interest of fluvoxamine as an add-on to clozapine in children with severe psychiatric disorder according to CYP polymorphisms: experience from a case series[J]. Front Psychiatry, 2021, 12: 669446.
XU J J, XIAO C F, PAN Y L, et al. Utilizing plasma drug levels and genetic testing to achieve optimal treatment response in a patient with treatment-resistant schizoaffective disorder[J]. Bipolar Disord, 2024, 26(1): 95-97.
BELLON A, NGUYEN K. Selective serotonin reuptake inhibitors and risk reduction for cardiovascular disease in patients with schizophrenia: a controversial but promising approach[J]. World J Psychiatry, 2021, 11(7): 316-324.
DE LEON J, RUAN C J, SCHORETSANITIS G, et al. A rational use of clozapine based on adverse drug reactions, pharmacokinetics, and clinical pharmacopsychology[J]. Psychother Psychosom, 2020, 89(4): 200-214.
DE LEON J, SCHORETSANITIS G, KANE J M, et al. Using therapeutic drug monitoring to personalize clozapine dosing in Asians[J]. Asia Pac Psychiatry, 2020, 12(2): e12384.
ROWLAND YEO K, GIL BERGLUND E, CHEN Y. Dose optimization informed by PBPK modeling: state-of-the art and future[J]. Clin Pharmacol Ther, 2024, 116(3): 563-576.
GILL J, MOULLET M, MARTINSSON A, et al. Comparing the applications of machine learning, PBPK, and population pharmacokinetic models in pharmacokinetic drug-drug interaction prediction[J]. CPT Pharmacometrics Syst Pharmacol, 2022, 11(12): 1560-1568.
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
1
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
2
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
1
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
1
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
0
1
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
1
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
0
1
... 氯氮平是难治性精神分裂症优先考虑的药物.氯氮平与其他药物联合使用时,可能会影响氯氮平的血药浓度,甚至会导致癫痫发作、代谢综合征等药物不良反应(adverse drug reaction,ADR)的发生[1-2].氟伏沙明是细胞色素P450成员1A2(cytochrome P450 1A2,CYP1A2)的强抑制剂,与氯氮平合用会发生药物-药物相互作用(drug-drug interaction,DDI),从而增加药物不良反应的发生风险[3-4].美国食品药品监督管理局(Food and Drug Administration,FDA)的药物标签建议合用氟伏沙明时减少氯氮平的剂量[5],该结论是针对高加索人群得出的,是否适用于中国群体尚无明确的证据[6-7].生理药物代谢动力学(physiologically based pharmacokinetic,PBPK)模型是药物代谢动力学研究的重要工具,能用于研究合并用药、种族等影响因素对药物体内给过程的影响[8-10].若能针对中国群体构建PBPK模型,对合用氟伏沙明后氯氮平的血药浓度进行预测,并以此为依据提出血药浓度剂量优化建议,可降低氯氮平的治疗风险[11-13]. ...
... Enzyme content of CYP450 subtypes in Chinese populationTab 1
CYP450
Sample 1[14]
Sample 2[15]
Sample 3[16]
WM
CYP1A2/(pmol·mg-1)
42.48
42.00
42.30
42.31
CYP2A6/(pmol·mg-1)
15.63
-
-
15.63
CYP2B6/(pmol·mg-1)
4.62
-
-
4.62
CYP2C9/(pmol·mg-1)
98.60
-
87.20
87.19
CYP2C19/(pmol·mg-1)
8.45
60.00
8.10
8.25
CYP2D6/(pmol·mg-1)
20.50
-
-
20.50
CYP2E1/(pmol·mg-1)
102.04
-
-
102.04
CYP3A4/(pmol·mg-1)
49.34
120.00
93.00/70.30
49.34
CYP3A5/(pmol·mg-1)
42.45
-
145.40/82.10
42.45
Note: Sample 1, Sample 2, and Sample 3 were from three clinical studies, each containing measurement data of CYP450 enzyme levels in the Chinese populations. CYP450—cytochrome P450; WM—weighted mean; “-” indicating missing data. ...
1
... Enzyme content of CYP450 subtypes in Chinese populationTab 1
CYP450
Sample 1[14]
Sample 2[15]
Sample 3[16]
WM
CYP1A2/(pmol·mg-1)
42.48
42.00
42.30
42.31
CYP2A6/(pmol·mg-1)
15.63
-
-
15.63
CYP2B6/(pmol·mg-1)
4.62
-
-
4.62
CYP2C9/(pmol·mg-1)
98.60
-
87.20
87.19
CYP2C19/(pmol·mg-1)
8.45
60.00
8.10
8.25
CYP2D6/(pmol·mg-1)
20.50
-
-
20.50
CYP2E1/(pmol·mg-1)
102.04
-
-
102.04
CYP3A4/(pmol·mg-1)
49.34
120.00
93.00/70.30
49.34
CYP3A5/(pmol·mg-1)
42.45
-
145.40/82.10
42.45
Note: Sample 1, Sample 2, and Sample 3 were from three clinical studies, each containing measurement data of CYP450 enzyme levels in the Chinese populations. CYP450—cytochrome P450; WM—weighted mean; “-” indicating missing data. ...
... Enzyme content of CYP450 subtypes in Chinese populationTab 1
CYP450
Sample 1[14]
Sample 2[15]
Sample 3[16]
WM
CYP1A2/(pmol·mg-1)
42.48
42.00
42.30
42.31
CYP2A6/(pmol·mg-1)
15.63
-
-
15.63
CYP2B6/(pmol·mg-1)
4.62
-
-
4.62
CYP2C9/(pmol·mg-1)
98.60
-
87.20
87.19
CYP2C19/(pmol·mg-1)
8.45
60.00
8.10
8.25
CYP2D6/(pmol·mg-1)
20.50
-
-
20.50
CYP2E1/(pmol·mg-1)
102.04
-
-
102.04
CYP3A4/(pmol·mg-1)
49.34
120.00
93.00/70.30
49.34
CYP3A5/(pmol·mg-1)
42.45
-
145.40/82.10
42.45
Note: Sample 1, Sample 2, and Sample 3 were from three clinical studies, each containing measurement data of CYP450 enzyme levels in the Chinese populations. CYP450—cytochrome P450; WM—weighted mean; “-” indicating missing data. ...



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}