上海交通大学学报(医学版) ›› 2021, Vol. 41 ›› Issue (12): 1580-1586.doi: 10.3969/j.issn.1674-8115.2021.12.006
吴志山1( ), 黄润2, 梁丽萍3, 朱宇婷2, 郑乔木1, 姜丽萍4()
), 黄润2, 梁丽萍3, 朱宇婷2, 郑乔木1, 姜丽萍4()
收稿日期:2020-12-18
出版日期:2021-12-28
发布日期:2021-01-28
通讯作者:
姜丽萍,电子信箱:13868311990@163.com。作者简介:吴志山(1994—),男,硕士生;电子信箱:zhishan0110@163.com。
基金资助:
Zhi-shan WU1(), Run HUANG2, Li-ping LIANG3, Yu-ting ZHU2, Qiao-mu ZHENG1, Li-ping JIANG4()
Received:2020-12-18
Online:2021-12-28
Published:2021-01-28
Contact:
JIANG Li-ping, E-mail: 13868311990@163.com.Supported by:摘要:
目的·了解重症监护病房(intensive care unit,ICU)老年患者术后谵妄发生的特征并分析其影响因素。方法·采用方便抽样法,选取2020年5月—9月入住上海交通大学医学院附属新华医院心胸外科ICU的老年术后患者作为研究对象。采用ICU意识模糊评估量表(Confusion Assessment Method-ICU,CAM-ICU)对患者进行谵妄评估。从患者手术结束转入ICU后开始评估,至术后第7日或转出ICU停止评估,记录患者谵妄发生情况。收集患者人口学及临床相关资料,并采用单因素分析和Logistic多因素回归分析探讨ICU老年患者术后谵妄的影响因素。结果·共纳入343例患者,103例发生术后谵妄,发生率为30.03%。谵妄发生时间在手术结束后7.5~130.0 h,平均为(47.4±29.7)h,中位数为35.5(23.0,61.0)h。谵妄发生在全天各时间段内分布均匀,仅术后24 h内谵妄昼夜发生时间存在集中趋势,高发时间为上午11:53,其他时间发生的谵妄昼夜分布无显著集中趋势。谵妄持续时间为6.5~131.0 h,平均为(32.4±28.1)h,中位数为20.5(14.0,45.0)h。单因素分析显示,谵妄组和无谵妄组患者的性别、糖尿病史、心功能分级、美国麻醉医师协会 (American Society of Anesthesiologists,ASA)麻醉分级、术中资料(手术时长、出血量、体外循环、低血压)、术后资料(机械通气、氧合指数)等差异有统计学意义(P<0.05)。多因素Logistic回归分析结果显示,ASA分级、术中低血压、术中体外循环对ICU老年患者术后谵妄有显著影响(均P<0.05)。结论·ICU老年患者术后谵妄发生率高,ASA分级高、术中低血压及术中体外循环是术后谵妄发生的影响因素。医护人员应了解其发生的特征及影响因素,加强谵妄评估并及时实施防治措施,以降低谵妄发生率、缩短谵妄持续时间。
中图分类号:
吴志山, 黄润, 梁丽萍, 朱宇婷, 郑乔木, 姜丽萍. ICU老年患者术后谵妄发生的特征及影响因素分析[J]. 上海交通大学学报(医学版), 2021, 41(12): 1580-1586.
Zhi-shan WU, Run HUANG, Li-ping LIANG, Yu-ting ZHU, Qiao-mu ZHENG, Li-ping JIANG. Characteristics and influencing factors of postoperative delirium among elderly patients in intensive care unit[J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2021, 41(12): 1580-1586.
| Item | Non-delirium group (n=240) | Delirium group (n=103) | t/Z/χ2 value | P value |
|---|---|---|---|---|
| Gender/n (%) | 3.894 | 0.048 | ||
| Male | 147 (61.3) | 74 (71.8) | ||
| Female | 93 (38.7) | 29 (28.2) | ||
| Age/year | 68.13±5.54 | 69.18±5.96 | -1.570 | 0.118 |
| BMI/n (%) | 1.335 | 0.513 | ||
| <18.5 (kg·m-2) | 19 (7.9) | 5 (4.9) | ||
| ≥18.5 and <24.0 (kg·m-2) | 120 (50.0) | 50 (48.5) | ||
| ≥24.0 (kg·m-2) | 101 (42.1) | 48 (46.6) | ||
| Smoking history/n (%) | 3.383 | 0.066 | ||
| Yes | 52 (21.7) | 32 (31.1) | ||
| No | 188 (78.3) | 71 (68.9) | ||
| Drinking history/n (%) | 0.249 | 0.618 | ||
| Yes | 23 (9.6) | 12 (11.7) | ||
| No | 217 (90.4) | 91 (88.3) | ||
| Hypertension/n (%) | 0.847 | 0.646 | ||
| Yes | 127 (52.9) | 59 (57.3) | ||
| No | 113 (47.1) | 44 (42.7) | ||
| Diabetes/n (%) | 4.033 | 0.045 | ||
| Yes | 40 (16.7) | 28 (27.2) | ||
| No | 200 (83.3) | 75 (72.8) | ||
| Stroke/n (%) | 2.243 | 0.134 | ||
| Yes | 27 (11.2) | 19 (18.4) | ||
| No | 213 (88.8) | 84 (81.6) | ||
| Kinds of drug/n (%) | 0.015 | 0.902 | ||
| <5 | 220 (91.7) | 94 (91.3) | ||
| ≥5 | 20 (8.3) | 9 (8.7) | ||
| Prealbumin/(mg·L-1) | 225.51±56.97 | 226.05±61.28 | 0.380 | 0.704 |
| Albumin/(g·L-1) | 41.83±7.24 | 40.46±4.07 | 1.785 | 0.075 |
| Cardiac function/n (%) | 14.328 | 0.000 | ||
| <Ⅲ | 180 (75.0) | 56 (54.4) | ||
| ≥Ⅲ | 60 (25.0) | 47 (45.6) | ||
| ASA/n (%) | 25.389 | 0.000 | ||
| Ⅱ | 97 (40.4) | 14 (13.6) | ||
| Ⅲ | 110 (45.8) | 62 (60.2) | ||
| Ⅳ | 33 (13.8) | 27 (26.2) | ||
| Operation duration/min | 196.44±87.68 | 233.49±79.98 | -3.674 | 0.001 |
| Intraoperative blood loss/mL | 100 (50, 200) | 200 (95, 300) | -3.776 | 0.000 |
| Cardiopulmonary bypass/n (%) | 18.050 | 0.000 | ||
| Yes | 40 (16.7) | 40 (38.8) | ||
| No | 200 (83.3) | 63 (61.2) | ||
| Intraoperative hypotension/n (%) | 30.616 | 0.000 | ||
| Yes | 60 (25.0) | 57 (55.3) | ||
| No | 180 (75.0) | 46 (44.7) | ||
| Mechanical ventilation/n (%) | 8.579 | 0.003 | ||
| Yes | 175 (72.9) | 90 (87.4) | ||
| No | 65 (27.1) | 13 (12.6) | ||
| Oxygenation index/mmHg | 316.94±119.26 | 259.27±128.51 | 4.037 | 0.000 |
| Lactic acid/(mg·L-1) | 2.70 (2.20, 3.80) | 2.90 (2.10, 4.00) | -1.065 | 0.287 |
表1 术后谵妄组与非谵妄组患者相关资料的比较(n=343)
Tab 1 Comparison of relevant factors between postoperative delirium and non-delirium patients (n=343)
| Item | Non-delirium group (n=240) | Delirium group (n=103) | t/Z/χ2 value | P value |
|---|---|---|---|---|
| Gender/n (%) | 3.894 | 0.048 | ||
| Male | 147 (61.3) | 74 (71.8) | ||
| Female | 93 (38.7) | 29 (28.2) | ||
| Age/year | 68.13±5.54 | 69.18±5.96 | -1.570 | 0.118 |
| BMI/n (%) | 1.335 | 0.513 | ||
| <18.5 (kg·m-2) | 19 (7.9) | 5 (4.9) | ||
| ≥18.5 and <24.0 (kg·m-2) | 120 (50.0) | 50 (48.5) | ||
| ≥24.0 (kg·m-2) | 101 (42.1) | 48 (46.6) | ||
| Smoking history/n (%) | 3.383 | 0.066 | ||
| Yes | 52 (21.7) | 32 (31.1) | ||
| No | 188 (78.3) | 71 (68.9) | ||
| Drinking history/n (%) | 0.249 | 0.618 | ||
| Yes | 23 (9.6) | 12 (11.7) | ||
| No | 217 (90.4) | 91 (88.3) | ||
| Hypertension/n (%) | 0.847 | 0.646 | ||
| Yes | 127 (52.9) | 59 (57.3) | ||
| No | 113 (47.1) | 44 (42.7) | ||
| Diabetes/n (%) | 4.033 | 0.045 | ||
| Yes | 40 (16.7) | 28 (27.2) | ||
| No | 200 (83.3) | 75 (72.8) | ||
| Stroke/n (%) | 2.243 | 0.134 | ||
| Yes | 27 (11.2) | 19 (18.4) | ||
| No | 213 (88.8) | 84 (81.6) | ||
| Kinds of drug/n (%) | 0.015 | 0.902 | ||
| <5 | 220 (91.7) | 94 (91.3) | ||
| ≥5 | 20 (8.3) | 9 (8.7) | ||
| Prealbumin/(mg·L-1) | 225.51±56.97 | 226.05±61.28 | 0.380 | 0.704 |
| Albumin/(g·L-1) | 41.83±7.24 | 40.46±4.07 | 1.785 | 0.075 |
| Cardiac function/n (%) | 14.328 | 0.000 | ||
| <Ⅲ | 180 (75.0) | 56 (54.4) | ||
| ≥Ⅲ | 60 (25.0) | 47 (45.6) | ||
| ASA/n (%) | 25.389 | 0.000 | ||
| Ⅱ | 97 (40.4) | 14 (13.6) | ||
| Ⅲ | 110 (45.8) | 62 (60.2) | ||
| Ⅳ | 33 (13.8) | 27 (26.2) | ||
| Operation duration/min | 196.44±87.68 | 233.49±79.98 | -3.674 | 0.001 |
| Intraoperative blood loss/mL | 100 (50, 200) | 200 (95, 300) | -3.776 | 0.000 |
| Cardiopulmonary bypass/n (%) | 18.050 | 0.000 | ||
| Yes | 40 (16.7) | 40 (38.8) | ||
| No | 200 (83.3) | 63 (61.2) | ||
| Intraoperative hypotension/n (%) | 30.616 | 0.000 | ||
| Yes | 60 (25.0) | 57 (55.3) | ||
| No | 180 (75.0) | 46 (44.7) | ||
| Mechanical ventilation/n (%) | 8.579 | 0.003 | ||
| Yes | 175 (72.9) | 90 (87.4) | ||
| No | 65 (27.1) | 13 (12.6) | ||
| Oxygenation index/mmHg | 316.94±119.26 | 259.27±128.51 | 4.037 | 0.000 |
| Lactic acid/(mg·L-1) | 2.70 (2.20, 3.80) | 2.90 (2.10, 4.00) | -1.065 | 0.287 |

图1 谵妄发生距离手术结束的时间分布
Fig 1 Distribution of delirium onset time from the end of surgery
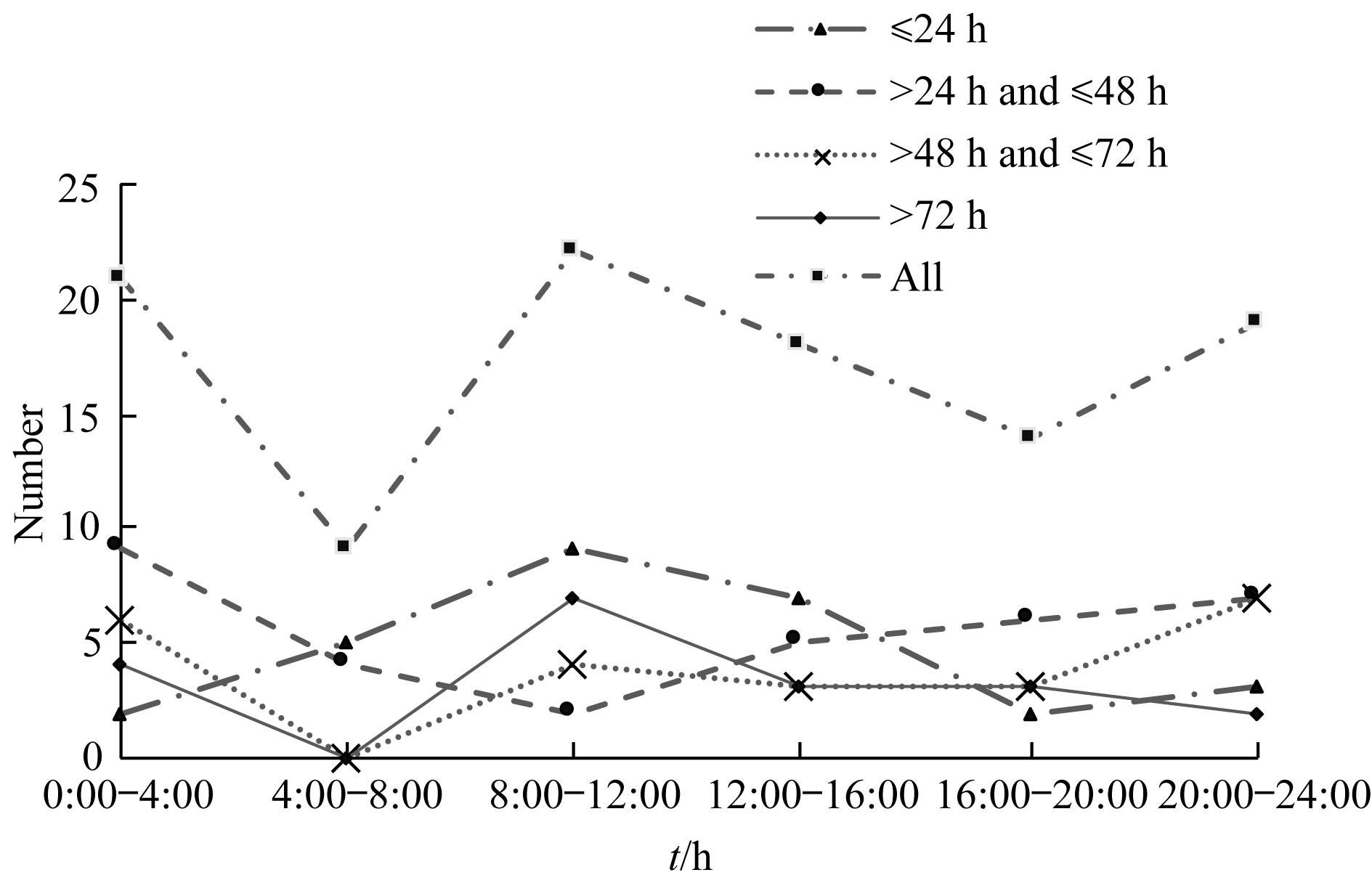
图2 谵妄发生昼夜时间分布
Fig 2 Distribution of delirium onset time in one day
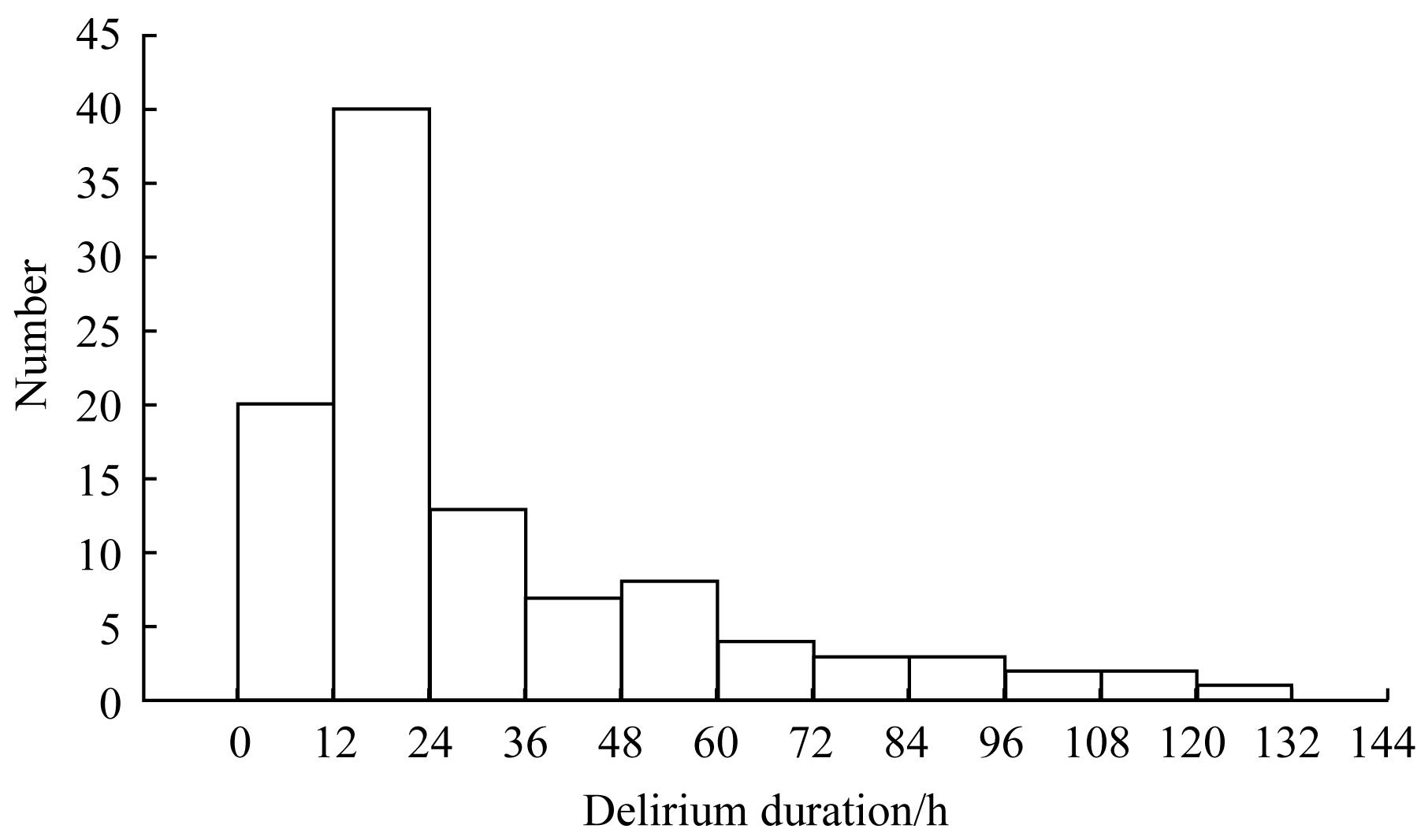
图3 谵妄持续时间分布
Fig 3 Distribution of delirium duration
| Variable | Assignment instruction |
|---|---|
| Gender | Male=0; Female=1 |
| Diabetes | No=0; Yes=1 |
| Cardiac function | <Ⅲ(Ⅰ、Ⅱ)=0; ≥Ⅲ(Ⅲ、Ⅳ)=1 |
| ASA classification | Ⅱ=1(reference group); Ⅲ=2; Ⅳ=3 |
| Operation duration | Original value |
| Intraoperative blood loss | Original value |
| Intraoperative hypotension | No=0; Yes=1 |
| Cardiopulmonary bypass | No=0; Yes=1 |
| Mechanical ventilation | No=0; Yes=1 |
| Oxygenation index | Original value |
表2 多因素分析自变量赋值
Tab 2 Assignment of independent variables in multivariate analysis
| Variable | Assignment instruction |
|---|---|
| Gender | Male=0; Female=1 |
| Diabetes | No=0; Yes=1 |
| Cardiac function | <Ⅲ(Ⅰ、Ⅱ)=0; ≥Ⅲ(Ⅲ、Ⅳ)=1 |
| ASA classification | Ⅱ=1(reference group); Ⅲ=2; Ⅳ=3 |
| Operation duration | Original value |
| Intraoperative blood loss | Original value |
| Intraoperative hypotension | No=0; Yes=1 |
| Cardiopulmonary bypass | No=0; Yes=1 |
| Mechanical ventilation | No=0; Yes=1 |
| Oxygenation index | Original value |
| Item | β | SE | Wald χ2 | P value | OR | 95%CI |
|---|---|---|---|---|---|---|
| Intraoperative hypotension | 1.273 | 0.261 | 23.775 | 0.000 | 3.573 | 2.142‒5.962 |
| Cardiopulmonary bypass | 0.729 | 0.291 | 6.290 | 0.012 | 2.073 | 1.173‒3.666 |
| ASA(Ⅱ) | ‒ | ‒ | 15.068 | 0.001 | 1.000 | ‒ |
| ASA(Ⅲ) | 1.216 | 0.343 | 12.547 | 0.000 | 3.373 | 1.721‒6.609 |
| ASA(Ⅳ) | 1.455 | 0.416 | 12.199 | 0.000 | 4.283 | 1.893‒9.687 |
| Constant | -2.499 | 0.324 | 59.482 | 0.000 | 0.082 | ‒ |
表3 ICU老年患者术后谵妄影响因素的多因素Logistic回归分析
Tab 3 Multivariate Logistic regression analysis of risk factors of postoperative delirium in elderly ICU patients
| Item | β | SE | Wald χ2 | P value | OR | 95%CI |
|---|---|---|---|---|---|---|
| Intraoperative hypotension | 1.273 | 0.261 | 23.775 | 0.000 | 3.573 | 2.142‒5.962 |
| Cardiopulmonary bypass | 0.729 | 0.291 | 6.290 | 0.012 | 2.073 | 1.173‒3.666 |
| ASA(Ⅱ) | ‒ | ‒ | 15.068 | 0.001 | 1.000 | ‒ |
| ASA(Ⅲ) | 1.216 | 0.343 | 12.547 | 0.000 | 3.373 | 1.721‒6.609 |
| ASA(Ⅳ) | 1.455 | 0.416 | 12.199 | 0.000 | 4.283 | 1.893‒9.687 |
| Constant | -2.499 | 0.324 | 59.482 | 0.000 | 0.082 | ‒ |
| 1 | 汤铂, 王小亭, 陈文劲, 等. 重症患者谵妄管理专家共识[J]. 中华内科杂志, 2019, 58(2): 108-118. |
| 2 | Li X, Zhang LN, Gong F, et al. Incidence and risk factors for delirium in older patients following intensive care unit admission: a prospective observational study[J]. J Nurs Res, 2020, 28(4): e101. |
| 3 | Pavone KJ, Jablonski J, Junker P, et al. Evaluating delirium outcomes among older adults in the surgical intensive care unit[J]. Heart Lung, 2020, 49(5): 578-584. |
| 4 | Kirfel A, Menzenbach J, Guttenthaler V, et al. Postoperative delirium after cardiac surgery of elderly patients as an independent risk factor for prolonged length of stay in intensive care unit and in hospital[J]. Aging Clin Exp Res, 2021. DOI: 10.1007/s40520-021-01842-x. |
| 5 | Bryczkowski SB, Lopreiato MC, Yonclas PP, et al. Risk factors for delirium in older trauma patients admitted to the surgical intensive care unit[J]. J Trauma Acute Care Surg, 2014, 77(6): 944-951. |
| 6 | Gaete OD, Papathanassoglou E, Norris CM. The lived experience of delirium in intensive care unit patients: a meta-ethnography[J]. Aust Crit Care, 2020, 33(2): 193-202. |
| 7 | Day J, Higgins I. Existential absence: the lived experience of family members during their older loved one's delirium[J]. Qual Health Res, 2015, 25(12): 1700-1718. |
| 8 | 潘燕彬, 颜建龙, 骆谏英, 等. 谵妄患者远期预后的研究进展[J]. 中华护理杂志, 2019, 54(9): 1415-1418. |
| 9 | Shi SM, Sung M, Afilalo J, et al. Delirium incidence and functional outcomes after transcatheter and surgical aortic valve replacement[J]. J Am Geriatr Soc, 2019, 67(7): 1393-1401. |
| 10 | 张海涛, 唐远志, 秦颖. 60岁以上结直肠癌患者术后谵妄的危险因素和临床结局[J]. 中华胃肠外科杂志, 2017, 20(11): 1263-1268. |
| 11 | Salluh JI, Wang H, Schneider EB, et al. Outcome of delirium in critically ill patients: systematic review and meta-analysis[J]. BMJ, 2015, 350: h2538. |
| 12 | Bijker JB, van Klei WA, Kappen TH, et al. Incidence of intraoperative hypotension as a function of the chosen definition: literature definitions applied to a retrospective cohort using automated data collection[J]. Anesthesiology, 2007, 107(2): 213-220. |
| 13 | Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU)[J]. JAMA, 2001, 286(21): 2703-2710. |
| 14 | 邹姮婧. 中文版CAM-ICU的信度效度检验及与其他量表的比较[D]. 武汉: 华中科技大学, 2012. |
| 15 | Velayati A, Vahdat SM, Shahbazi E, et al. Association between preoperative nutritional status and postoperative delirium in individuals with coronary artery bypass graft surgery: a prospective cohort study[J]. Nutrition, 2019, 66: 227-232. |
| 16 | Järvelä K, Porkkala H, Karlsson S, et al. Postoperative delirium in cardiac surgery patients[J]. J Cardiothorac Vasc Anesth, 2018, 32(4): 1597-1602. |
| 17 | 张竞超, 张丁恺, 郭龙辉, 等. 心脏外科手术后谵妄的危险因素分析[J]. 中华胸心血管外科杂志, 2019, 35(1): 29-32. |
| 18 | Kochunov P, Ramage AE, Lancaster JL, et al. Loss of cerebral white matter structural integrity tracks the gray matter metabolic decline in normal aging[J]. Neuroimage, 2009, 45(1): 17-28. |
| 19 | Kelly KM, Nadon NL, Morrison JH, et al. The neurobiology of aging[J]. Epilepsy Res, 2006: 68(): S5-S20. |
| 20 | Juraska JM, Lowry NC. Neuroanatomical changes associated with cognitive aging[J]. Curr Top Behav Neurosci, 2012, 10: 137-162. |
| 21 | Kazmierski J, Banys A, Latek J, et al. Cortisol levels and neuropsychiatric diagnosis as markers of postoperative delirium: a prospective cohort study[J]. Crit Care, 2013, 17(2): R38. |
| 22 | Maldonado JR. Delirium pathophysiology: an updated hypothesis of the etiology of acute brain failure[J]. Int J Geriatr Psychiatry, 2018, 33(11): 1428-1457. |
| 23 | Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU[J]. Crit Care Med, 2018, 46(9): e825-e873. |
| 24 | 中华医学会老年医学分会. 老年患者术后谵妄防治中国专家共识[J]. 中华老年医学杂志, 2016, 35(12): 1257-1262. |
| 25 | Lee H, Oh SY, Yu JH, et al. Risk factors of postoperative delirium in the intensive care unit after liver transplantation[J]. World J Surg, 2018, 42(9): 2992-2999. |
| 26 | Zhang W, Hu W, Shen M, et al. Profiles of delirium and the clinical outcomes of patients who underwent coronary artery bypass grafting: a prospective study from China[J]. J Clin Nurs, 2016, 25(5-6): 631-641. |
| 27 | Grover S, Kate N, Malhotra S, et al. Symptom profile of delirium in children and adolescent: does it differ from adults and elderly?[J]. Gen Hosp Psychiatry, 2012, 34(6): 626-632. |
| 28 | 刘春雪, 章洁, 邢攸红, 等. 急性心肌梗死并发谵妄的发作特点及其护理[J]. 解放军护理杂志, 2010, 27(16): 1241-1242, 1245. |
| 29 | Bellelli G, Carnevali L, Corsi M, et al. The impact of psychomotor subtypes and duration of delirium on 6-month mortality in hip-fractured elderly patients[J]. Int J Geriatr Psychiatry, 2018, 33(9): 1229-1235. |
| 30 | Lee H, Ju JW, Oh SY, et al. Impact of timing and duration of postoperative delirium: a retrospective observational study[J]. Surgery, 2018, 164(1): 137-143. |
| 31 | Khan BA, Perkins AJ, Prasad NK, et al. Biomarkers of delirium duration and delirium severity in the ICU[J]. Crit Care Med, 2020, 48(3): 353-361. |
| 32 | Cereghetti C, Siegemund M, Schaedelin S, et al. Independent predictors of the duration and overall burden of postoperative delirium after cardiac surgery in adults: an observational cohort study[J]. J Cardiothorac Vasc Anesth, 2017, 31(6): 1966-1973. |
| 33 | Janssen TL, Steyerberg EW, Faes MC, et al. Risk factors for postoperative delirium after elective major abdominal surgery in elderly patients: a cohort study[J]. Int J Surg, 2019, 71: 29-35. |
| 34 | Oldroyd C, Scholz AFM, Hinchliffe RJ, et al. A systematic review and meta-analysis of factors for delirium in vascular surgical patients[J]. J Vasc Surg, 2017, 66(4): 1269-1279.e9. |
| 35 | Sankar A, Johnson SR, Beattie WS, et al. Reliability of the American Society of Anesthesiologists physical status scale in clinical practice[J]. Br J Anaesth, 2014, 113(3): 424-432. |
| 36 | Giannice R, Foti E, Poerio A, et al. Perioperative morbidity and mortality in elderly gynecological oncological patients (≥70 years) by the American Society of Anesthesiologists physical status classes[J]. Ann Surg Oncol, 2004, 11(2): 219-225. |
| 37 | Siepe M, Pfeiffer T, Gieringer A, et al. Increased systemic perfusion pressure during cardiopulmonary bypass is associated with less early postoperative cognitive dysfunction and delirium[J]. Eur J Cardiothorac Surg, 2011, 40(1): 200-207. |
| 38 | Maheshwari K, Ahuja S, Khanna AK, et al. Association between perioperative hypotension and delirium in postoperative critically ill patients: a retrospective cohort analysis[J]. Anesth Analg, 2020, 130(3): 636-643. |
| 39 | Hirsch J, DePalma G, Tsai TT, et al. Impact of intraoperative hypotension and blood pressure fluctuations on early postoperative delirium after non-cardiac surgery[J]. Br J Anaesth, 2015, 115(3): 418-426. |
| 40 | Brady K, Hogue CW. Intraoperative hypotension and patient outcome: does "one size fit all?"[J]. Anesthesiology, 2013, 119(3): 495-497. |
| 41 | Siepe M, Pfeiffer T, Gieringer A, et al. Increased systemic perfusion pressure during cardiopulmonary bypass is associated with less early postoperative cognitive dysfunction and delirium[J]. Eur J Cardiothorac Surg, 2011, 40(1): 200-207. |
| 42 | Burkhart CS, Rossi A, Dell-Kuster S, et al. Effect of age on intraoperative cerebrovascular autoregulation and near-infrared spectroscopy-derived cerebral oxygenation[J]. Br J Anaesth, 2011, 107(5): 742-748. |
| 43 | Shadvar K, Baastani F, Mahmoodpoor A, et al. Evaluation of the prevalence and risk factors of delirium in cardiac surgery ICU[J]. J Cardiovasc Thorac Res, 2013, 5(4): 157-161. |
| 44 | 黄伟明, 周成斌. 体外循环新进展[M]. 北京: 人民卫生出版社, 2017. |
| 45 | Salameh A, Dhein S, Dähnert I, et al. Neuroprotective strategies during cardiac surgery with cardiopulmonary bypass[J]. Int J Mol Sci, 2016, 17(11): 1945. |
| 46 | Zakkar M, Guida G, Suleiman MS, et al. Cardiopulmonary bypass and oxidative stress[J]. Oxid Med Cell Longev, 2015, 2015: 189863. |
| [1] | 陆晔峰, 高磊青, 倪晓筱, 富晶晶. 儿童肝移植术后早期血糖及血脂的多时间点监测与影响因素分析[J]. 上海交通大学学报(医学版), 2025, 45(4): 443-451. |
| [2] | 陈佳莹, 褚以忞, 彭海霞. 结直肠癌无进展生存时间预测模型及影响因素研究[J]. 上海交通大学学报(医学版), 2025, 45(3): 324-334. |
| [3] | 陈丽红, 王妍, 周翔天, 郑俊克, 闫小响. 国家自然科学基金青年科学基金项目立项的影响因素分析——以上海交通大学医学院为例[J]. 上海交通大学学报(医学版), 2024, 44(9): 1205-1212. |
| [4] | 张懿熠, 倪长宇, 金迎, 何亚平, 冯楠楠. 高血压和血脂异常对城市老年居民认知影响的研究[J]. 上海交通大学学报(医学版), 2024, 44(7): 907-914. |
| [5] | 董冉, 余倩, 台瑞, 杨富, 方芳. 重症监护病房转出后患者早期症状网络分析[J]. 上海交通大学学报(医学版), 2024, 44(6): 733-740. |
| [6] | 郝明秀, 陈鸿伟, 王俊琳, 唐吟菡, 吴芸芸, 金玉华, 胡耀敏. 住院患者慢性病共病现状调查及流行病学分析[J]. 上海交通大学学报(医学版), 2024, 44(4): 462-468. |
| [7] | 傅艺玲, 吴茜, 罗晓庆, 吴艾泓, 夏雪兰, 郑敏. 晚期癌症患者预立医疗照护计划参与行为影响因素的系统综述[J]. 上海交通大学学报(医学版), 2024, 44(4): 482-493. |
| [8] | 王俊琳, 郝明秀, 唐吟菡, 吴芸芸, 金玉华, 胡耀敏. 慢性病共病、相位角与老年人肌少症相关的肌肉质量减少的关系研究[J]. 上海交通大学学报(医学版), 2024, 44(2): 196-203. |
| [9] | 蒋莹, 李清瑶, 陈之琦, 汪佳璐, 李云, 徐仁应. 老年人群体质量指数与慢性代谢性疾病的关系[J]. 上海交通大学学报(医学版), 2024, 44(2): 250-257. |
| [10] | 赵萌, 江莉婷, 高益鸣. 基于锥形线束CT的上颌后牙区牙槽骨增龄性变化研究[J]. 上海交通大学学报(医学版), 2024, 44(10): 1273-1278. |
| [11] | 罗晨, 沈玲, 王传伟, 顾佳妮, 王瑾, 赵黎, 黄帅. 腹腔镜结直肠癌根治术后患者早期下床活动现状及影响因素[J]. 上海交通大学学报(医学版), 2023, 43(9): 1201-1210. |
| [12] | 王晓玉, 彭银辉, 马文琳, 姚博爽, 李一凡, 赵莉, 杨春霞. 新冠疫情大流行期间儿童及青少年新发焦虑症状的纵向研究[J]. 上海交通大学学报(医学版), 2023, 43(8): 963-970. |
| [13] | 王雅玉, 蒋惠如, 叶梦月, 李萍, 袁安彩, 张薇, 卜军. 上海社区老年人群脑卒中与体力活动的关联性研究[J]. 上海交通大学学报(医学版), 2023, 43(11): 1348-1358. |
| [14] | 台瑞, 方芳, 毛晶珏, 周霞. 永久性肠造口患者造口适应水平影响因素分析[J]. 上海交通大学学报(医学版), 2023, 43(11): 1423-1429. |
| [15] | 刘秋利, 江来, 翁晓建. 老年患者全身麻醉术后肌松残余的研究进展[J]. 上海交通大学学报(医学版), 2023, 43(1): 108-113. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||