上海交通大学学报(医学版) ›› 2026, Vol. 46 ›› Issue (5): 612-623.doi: 10.3969/j.issn.1674-8115.2026.05.007
• 论著 · 临床研究 • 上一篇
刘智通, 樊子旭, 李想, 张敏( )
)
收稿日期:2025-11-24
接受日期:2026-01-19
出版日期:2026-05-28
发布日期:2026-05-28
通讯作者:
张 敏,主任医师,博士;电子信箱:zhangminxk@126.com。基金资助:
Liu Zhitong, Fan Zixu, Li Xiang, Zhang Min()
Received:2025-11-24
Accepted:2026-01-19
Online:2026-05-28
Published:2026-05-28
Contact:
Zhang Min, E-mail: zhangminxk@126.com.Supported by:摘要:
目的·探讨肺癌患者发生免疫检查点抑制剂相关心肌炎(immune checkpoint inhibitor-associated myocarditis,ICI-M)后,永久停药与继续免疫治疗的安全性差异。方法·采用单中心回顾性队列研究,纳入上海交通大学医学院附属胸科医院2016年6月至2024年8月确诊ICI-M的肺癌患者357例。根据ICI-M后的免疫治疗策略分为永久停药组(n=131)与继续治疗组(n=226)。继续治疗组包括从未停药患者以及暂时停药后重启患者。描述性统计ICI-M复发率及新发其他免疫相关不良事件(immune-related adverse events,irAEs)发生率,比较首次ICI-M与复发ICI-M的严重程度,并探索ICI-M复发或新发其他类型irAEs的危险因素。利用多因素Cox回归分析继续免疫治疗对主要心血管不良事件(major adverse cardiovascular events,MACE)的影响。采用倾向性评分匹配进行敏感性分析,以增强研究结果的稳健性。结果·ICI-M复发率为8.8%(20/226),复发ICI-M时的临床症状严重程度及心肌损伤标志物峰值并未高于首次ICI-M。13.3%(30/226)患者新发其他类型irAEs。ICI-M复发或新发其他类型irAEs的患者首次ICI-M发生时间更早(47.0 d vs 71.0 d,P=0.006),肌酸激酶同工酶MB(creatine kinase-MB,CK-MB)峰值更高(4.8 ng/mL vs 2.8 ng/mL,P=0.019)。多因素Cox回归显示,继续免疫治疗并未显著增加ICI-M患者的远期MACE发生风险(HR=0.75,95%CI 0.28~1.98,P=0.556),且该结果在各亚组中均保持一致(P相互作用>0.05)。采用倾向性评分匹配进行敏感性分析,结论依然保持稳健(匹配后HR=0.93,95%CI 0.32~2.70,P=0.894)。结论·肺癌患者发生ICI-M后继续免疫治疗总体安全性良好,ICI-M复发率较低,且继续免疫治疗并不显著增加MACE发生风险。研究结果为临床决策提供初步数据支持,未来仍需大规模前瞻性研究对结论加以确认与验证。
中图分类号:
刘智通, 樊子旭, 李想, 张敏. 肺癌患者免疫检查点抑制剂相关心肌炎后永久停药与继续免疫治疗的安全性比较[J]. 上海交通大学学报(医学版), 2026, 46(5): 612-623.
Liu Zhitong, Fan Zixu, Li Xiang, Zhang Min. Safety outcomes of immunotherapy continuation versus permanent discontinuation after immune checkpoint inhibitor-associated myocarditis in patients with lung cancer[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(5): 612-623.
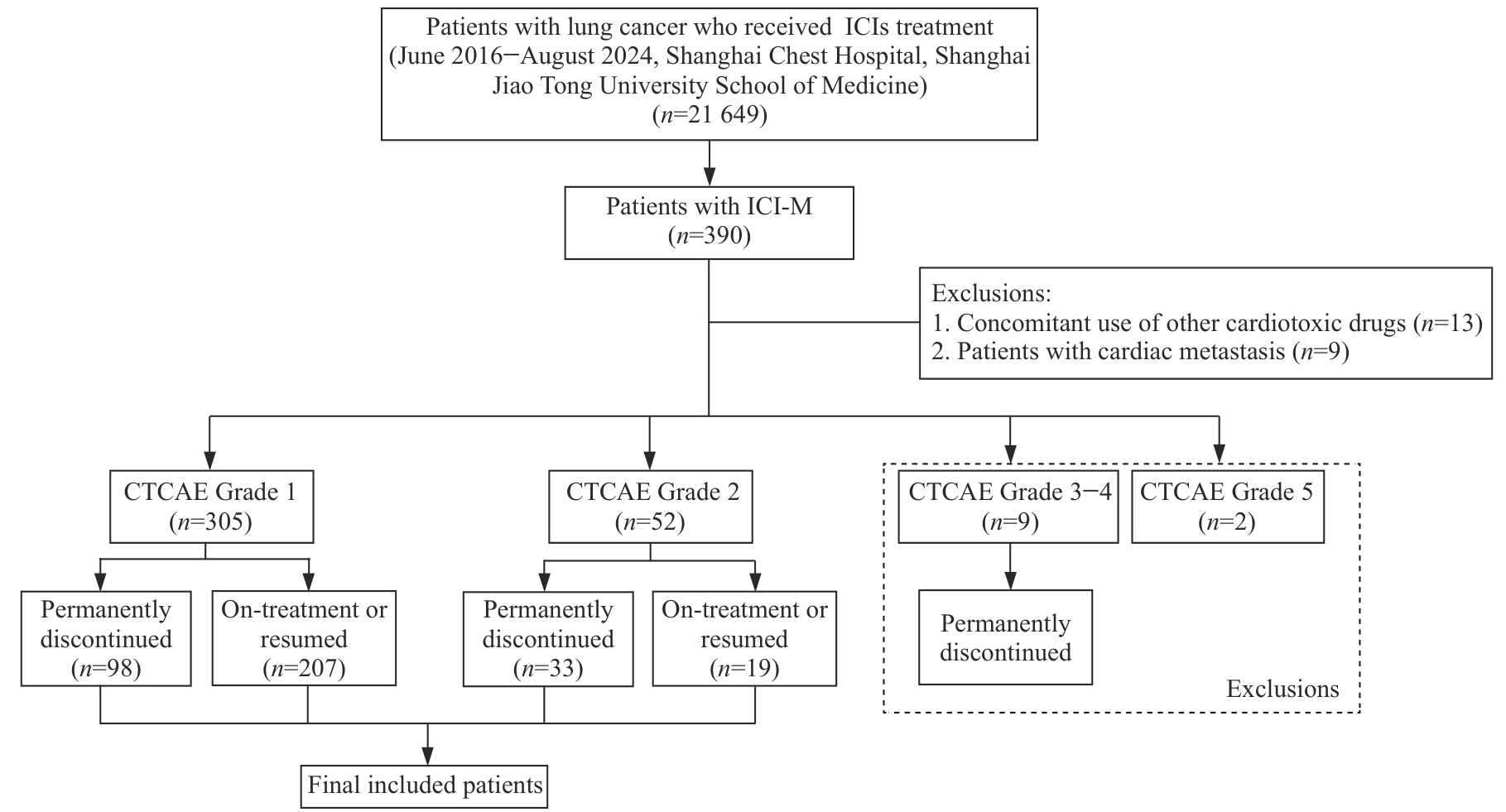
图1 研究设计流程图
Fig 1 Flowchart of the study design
| Characteristic | CTCAE Grade 1 (n=305) | CTCAE Grade 2 (n=52) | P value | ||
|---|---|---|---|---|---|
| On-treatment or resumed (n=207) | Permanently discontinued (n=98) | On-treatment or resumed (n=19) | Permanently discontinued (n=33) | ||
| Clinical characteristic | |||||
| Age/year | 67.0 (61.0, 71.0) | 68.0 (61.0, 73.0) | 64.0 (61.0, 72.0) | 66.0 (62.0, 69.0) | 0.593 |
| Male/n(%) | 185 (89.4) | 74 (75.5) | 16 (84.2) | 27 (81.8) | 0.018 |
| BMI/(kg·m-2) | 22.6 (20.3, 24.7) | 22.5 (20.4, 24.9) | 23.1 (21.0, 24.5) | 22.9 (22.2, 25.6) | 0.392 |
| Coronary artery disease/n(%) | 33 (15.9) | 16 (16.3) | 6 (31.6) | 10 (30.3) | 0.091 |
| Hyperlipidemia/n(%) | 13 (6.3) | 7 (7.1) | 1 (5.3) | 3 (9.1) | 0.929 |
| Hypertension/n(%) | 77 (37.2) | 35 (35.7) | 4 (21.1) | 10 (30.3) | 0.497 |
| Diabetes/n(%) | 26 (12.6) | 13 (13.3) | 3 (15.8) | 6 (18.2) | 0.832 |
| Chronic kidney disease/n(%) | 5 (2.4) | 4 (4.1) | 0 (0) | 1 (3.3) | 0.739 |
| Histology/n(%) | 0.583 | ||||
| Squamous cell carcinoma | 74 (35.7) | 30 (30.6) | 7 (36.8) | 10 (30.3) | |
| Adenocarcinoma | 84 (40.6) | 47 (48.0) | 8 (42.1) | 14 (42.4) | |
| Other NSCLC | 26 (12.6) | 7 (7.1) | 2 (10.5) | 7 (21.2) | |
| SCLC | 23 (11.1) | 14 (14.3) | 2 (10.5) | 2 (6.1) | |
| Disease stage/n(%) | 0.265 | ||||
| Stage Ⅱ‒Ⅲ | 78 (37.7) | 28 (28.6) | 4 (21.1) | 11 (33.3) | |
| Stage Ⅳ | 129 (62.3) | 70 (71.4) | 15 (78.9) | 22 (66.7) | |
| ECOG performance status①/n(%) | 0.072 | ||||
| 0 | 24 (14.3) | 4 (5.2) | 0 (0) | 3 (12.5) | |
| 1 | 143 (85.1) | 71 (92.2) | 9 (90.0) | 20 (83.3) | |
| 2 | 1 (0.6) | 2 (2.6) | 1 (10.0) | 1 (4.2) | |
| Baseline laboratory test | |||||
| Hemoglobin/(g·L-1) | 129.0 (116.0, 141.0) | 126.5 (115.0, 139.0) | 132.0 (128.0, 144.0) | 127.0 (116.0, 139.0) | 0.550 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 41.0 (38.0, 42.0) | 39.0 (37.0, 42.0) | 0.794 |
| HbA1c/% | 5.8 (5.6, 6.3) | 5.8 (5.3, 6.5) | 5.8 (5.3, 6.7) | 6.0 (5.7, 6.2) | 0.803 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.8 (85.9, 101.1) | 94.3 (77.8, 100.9) | 99.0 (85.9, 103.4) | 91.5 (78.3, 95.9) | 0.237 |
| Anti-tumor therapy | |||||
| Radiotherapy/n(%) | 67 (32.4) | 33 (33.7) | 7 (36.8) | 11 (33.3) | 0.980 |
| Initial ICI type/n(%) | 0.522 | ||||
| PD-1i monotherapy | 170 (82.1) | 83 (84.7) | 18 (94.7) | 29 (87.9) | |
| PD-L1i monotherapy | 29 (14.0) | 14 (14.3) | 1 (5.3) | 4 (12.1) | |
| Combination therapy | 8 (3.9) | 1 (1.0) | 0 (0) | 0 (0) | |
| Number of cycles received prior to ICI-M | 2.0 (1.0, 5.0) | 3.0 (2.0, 6.0) | 3.0 (2.0, 7.5) | 2.0 (1.0, 3.0) | 0.131 |
| Ongoing treatment/n(%) | 0.184 | ||||
| ICIs monotherapy | 42 (20.3) | 16 (16.3) | 7 (36.8) | 7 (21.2) | |
| Combination with chemotherapy | 138 (66.7) | 69 (70.4) | 10 (52.6) | 20 (60.6) | |
| Combination with targeted therapy | 17 (8.2) | 8 (8.2) | 0 (0) | 1 (3.0) | |
| Combination with chemotherapy and targeted therapy | 10 (4.8) | 5 (5.1) | 2 (10.5) | 5 (15.2) | |
| Clinical characteristics of initial ICI-M | |||||
| Time to initial ICI-M/month | 2.0 (1.0, 5.0) | 3.0 (1.0, 6.0) | 3.0 (1.0, 7.5) | 2.0 (1.0, 3.0) | 0.073 |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 140.0) | 90.0 (60.0, 190.0) | 310.0 (130.0, 550.0) | 390.0 (120.0, 610.0) | <0.001 |
| Peak CK-MB/(ng·mL-1) | 3.0 (1.8, 6.3) | 3.5 (1.8, 12.1) | 4.4 (2.8, 10.1) | 11.0 (3.5, 73.7) | <0.001 |
| Management/n(%) | |||||
| Hospitalization | 17 (8.2) | 24 (24.5) | 11 (57.9) | 22 (66.7) | <0.001 |
| Systemic steroids use | 13 (6.3) | 25 (25.5) | 3 (15.8) | 21 (63.6) | <0.001 |
表1 ICI-M患者临床基线特征
Tab 1 Baseline characteristics of patients with ICI-M
| Characteristic | CTCAE Grade 1 (n=305) | CTCAE Grade 2 (n=52) | P value | ||
|---|---|---|---|---|---|
| On-treatment or resumed (n=207) | Permanently discontinued (n=98) | On-treatment or resumed (n=19) | Permanently discontinued (n=33) | ||
| Clinical characteristic | |||||
| Age/year | 67.0 (61.0, 71.0) | 68.0 (61.0, 73.0) | 64.0 (61.0, 72.0) | 66.0 (62.0, 69.0) | 0.593 |
| Male/n(%) | 185 (89.4) | 74 (75.5) | 16 (84.2) | 27 (81.8) | 0.018 |
| BMI/(kg·m-2) | 22.6 (20.3, 24.7) | 22.5 (20.4, 24.9) | 23.1 (21.0, 24.5) | 22.9 (22.2, 25.6) | 0.392 |
| Coronary artery disease/n(%) | 33 (15.9) | 16 (16.3) | 6 (31.6) | 10 (30.3) | 0.091 |
| Hyperlipidemia/n(%) | 13 (6.3) | 7 (7.1) | 1 (5.3) | 3 (9.1) | 0.929 |
| Hypertension/n(%) | 77 (37.2) | 35 (35.7) | 4 (21.1) | 10 (30.3) | 0.497 |
| Diabetes/n(%) | 26 (12.6) | 13 (13.3) | 3 (15.8) | 6 (18.2) | 0.832 |
| Chronic kidney disease/n(%) | 5 (2.4) | 4 (4.1) | 0 (0) | 1 (3.3) | 0.739 |
| Histology/n(%) | 0.583 | ||||
| Squamous cell carcinoma | 74 (35.7) | 30 (30.6) | 7 (36.8) | 10 (30.3) | |
| Adenocarcinoma | 84 (40.6) | 47 (48.0) | 8 (42.1) | 14 (42.4) | |
| Other NSCLC | 26 (12.6) | 7 (7.1) | 2 (10.5) | 7 (21.2) | |
| SCLC | 23 (11.1) | 14 (14.3) | 2 (10.5) | 2 (6.1) | |
| Disease stage/n(%) | 0.265 | ||||
| Stage Ⅱ‒Ⅲ | 78 (37.7) | 28 (28.6) | 4 (21.1) | 11 (33.3) | |
| Stage Ⅳ | 129 (62.3) | 70 (71.4) | 15 (78.9) | 22 (66.7) | |
| ECOG performance status①/n(%) | 0.072 | ||||
| 0 | 24 (14.3) | 4 (5.2) | 0 (0) | 3 (12.5) | |
| 1 | 143 (85.1) | 71 (92.2) | 9 (90.0) | 20 (83.3) | |
| 2 | 1 (0.6) | 2 (2.6) | 1 (10.0) | 1 (4.2) | |
| Baseline laboratory test | |||||
| Hemoglobin/(g·L-1) | 129.0 (116.0, 141.0) | 126.5 (115.0, 139.0) | 132.0 (128.0, 144.0) | 127.0 (116.0, 139.0) | 0.550 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 41.0 (38.0, 42.0) | 39.0 (37.0, 42.0) | 0.794 |
| HbA1c/% | 5.8 (5.6, 6.3) | 5.8 (5.3, 6.5) | 5.8 (5.3, 6.7) | 6.0 (5.7, 6.2) | 0.803 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.8 (85.9, 101.1) | 94.3 (77.8, 100.9) | 99.0 (85.9, 103.4) | 91.5 (78.3, 95.9) | 0.237 |
| Anti-tumor therapy | |||||
| Radiotherapy/n(%) | 67 (32.4) | 33 (33.7) | 7 (36.8) | 11 (33.3) | 0.980 |
| Initial ICI type/n(%) | 0.522 | ||||
| PD-1i monotherapy | 170 (82.1) | 83 (84.7) | 18 (94.7) | 29 (87.9) | |
| PD-L1i monotherapy | 29 (14.0) | 14 (14.3) | 1 (5.3) | 4 (12.1) | |
| Combination therapy | 8 (3.9) | 1 (1.0) | 0 (0) | 0 (0) | |
| Number of cycles received prior to ICI-M | 2.0 (1.0, 5.0) | 3.0 (2.0, 6.0) | 3.0 (2.0, 7.5) | 2.0 (1.0, 3.0) | 0.131 |
| Ongoing treatment/n(%) | 0.184 | ||||
| ICIs monotherapy | 42 (20.3) | 16 (16.3) | 7 (36.8) | 7 (21.2) | |
| Combination with chemotherapy | 138 (66.7) | 69 (70.4) | 10 (52.6) | 20 (60.6) | |
| Combination with targeted therapy | 17 (8.2) | 8 (8.2) | 0 (0) | 1 (3.0) | |
| Combination with chemotherapy and targeted therapy | 10 (4.8) | 5 (5.1) | 2 (10.5) | 5 (15.2) | |
| Clinical characteristics of initial ICI-M | |||||
| Time to initial ICI-M/month | 2.0 (1.0, 5.0) | 3.0 (1.0, 6.0) | 3.0 (1.0, 7.5) | 2.0 (1.0, 3.0) | 0.073 |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 140.0) | 90.0 (60.0, 190.0) | 310.0 (130.0, 550.0) | 390.0 (120.0, 610.0) | <0.001 |
| Peak CK-MB/(ng·mL-1) | 3.0 (1.8, 6.3) | 3.5 (1.8, 12.1) | 4.4 (2.8, 10.1) | 11.0 (3.5, 73.7) | <0.001 |
| Management/n(%) | |||||
| Hospitalization | 17 (8.2) | 24 (24.5) | 11 (57.9) | 22 (66.7) | <0.001 |
| Systemic steroids use | 13 (6.3) | 25 (25.5) | 3 (15.8) | 21 (63.6) | <0.001 |
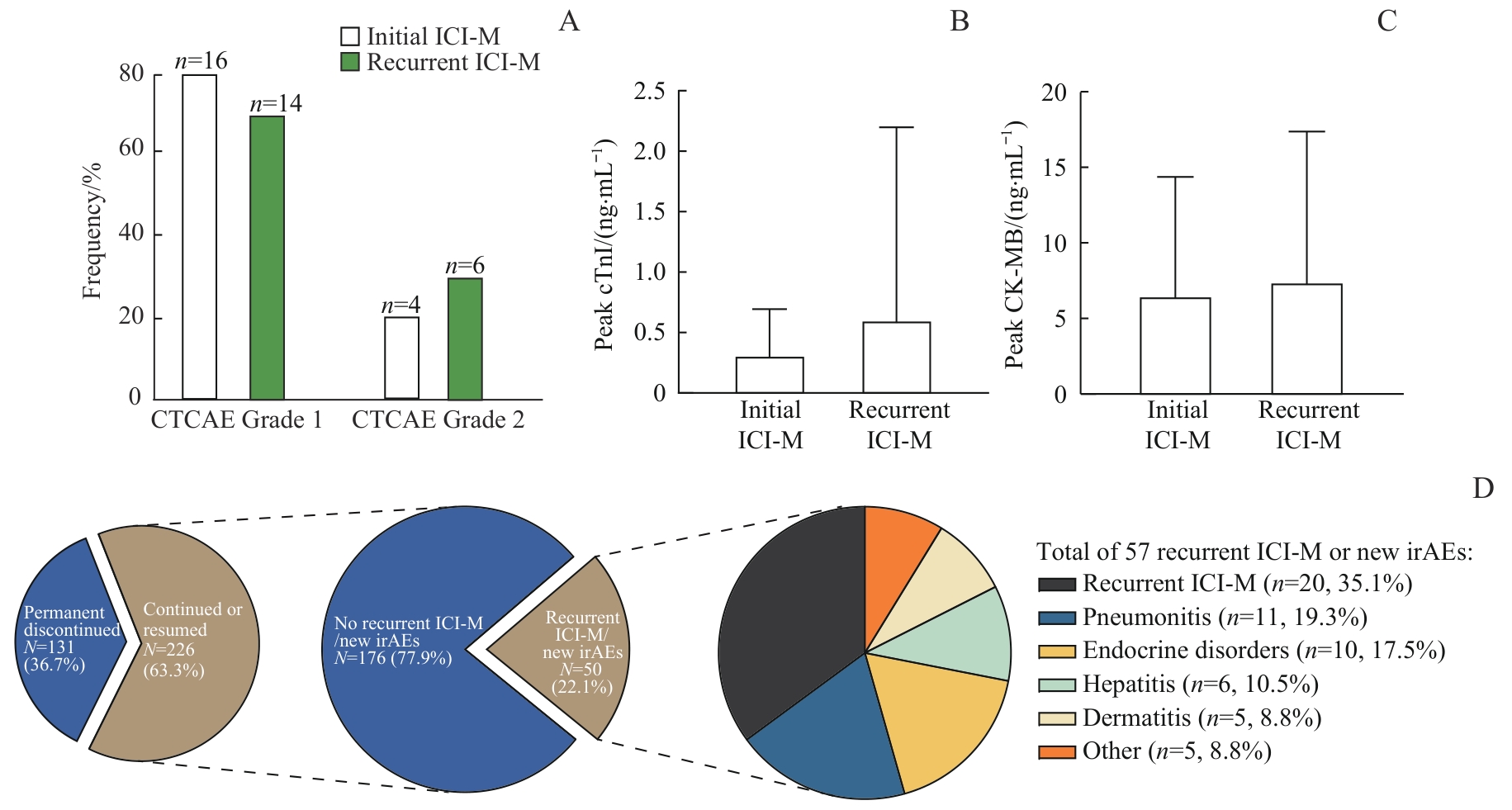
图2 复发ICI-M及新发其他类型irAEs的临床特征Note: A‒C. Comparison of CTCAE grades (A), peak cTnI levels (B), and peak CK-MB levels (C) between initial and recurrent ICI-M. D. Incidence of recurrent ICI-M and other new-onset irAEs. As some patients experienced multiple irAEs, a total of 57 irAEs were recorded in 50 patients.
Fig 2 Clinical characteristics of recurrent ICI-M and new-onset irAEs
| Variable | No recurrent ICI-M/new irAEs (n=176) | Recurrent ICI-M/new irAEs (n=50) | P value |
|---|---|---|---|
| Age/year | 67.0 (61.0, 71.0) | 67.0 (62.0, 73.0) | 0.535 |
| Male/n(%) | 157 (89.2) | 44 (88.0) | 1.000 |
| BMI/(kg·m-2) | 22.9 ± 3.4 | 22.5 ± 3.3 | 0.483 |
| Coronary artery disease/n(%) | 28 (15.9) | 11 (22.0) | 0.427 |
| Hyperlipidemia/n(%) | 9 (5.1) | 5 (10.0) | 0.351 |
| Hypertension/n(%) | 63 (35.8) | 18 (36.0) | 1.000 |
| Diabetes/n(%) | 23 (13.1) | 6 (12.0) | 1.000 |
| Chronic kidney disease/n(%) | 2 (1.1) | 3 (6.0) | 0.129 |
| Histology/n(%) | 0.788 | ||
| Squamous cell carcinoma | 64 (36.4) | 17 (34.0) | |
| Adenocarcinoma | 69 (39.2) | 23 (46.0) | |
| Other NSCLC | 22 (12.5) | 6 (12.0) | |
| SCLC | 21 (11.9) | 4 (8.0) | |
| Disease stage/n(%) | 0.146 | ||
| Stage Ⅱ‒Ⅲ | 59 (33.5) | 23 (46.0) | |
| Stage Ⅳ | 117 (66.5) | 27 (54.0) | |
| ECOG performance status①/n(%) | 0.459 | ||
| 0 | 20 (14.8) | 4 (9.3) | |
| 1 | 113 (83.7) | 39 (90.7) | |
| 2 | 2 (1.5) | 0 (0) | |
| Hemoglobin/(g·L-1) | 130.0 (116.0, 140.5) | 128.5 (118.0, 142.0) | 0.951 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 0.366 |
| HbA1c/% | 5.8 (5.5, 6.3) | 5.8 (5.7, 6.3) | 0.384 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.9 (86.3, 101.3) | 94.1 (81.6, 101.2) | 0.655 |
| Radiotherapy/n(%) | 58 (33.0) | 16 (32.0) | 1.000 |
| ICI type after initial ICI-M/n(%) | 1.000 | ||
| PD-1 monotherapy | 150 (85.2) | 43 (86.0) | |
| PD-L1 monotherapy | 26 (14.8) | 7 (14.0) | |
| Anti-tumor treatment after initial ICI-M/n(%) | 0.244 | ||
| ICIs monotherapy | 45 (25.6) | 15 (30.0) | |
| Combination with chemotherapy | 109 (61.9) | 27 (54.0) | |
| Combination with targeted therapy | 12 (6.8) | 7 (14.0) | |
| Combination with chemotherapy and targeted therapy | 10 (5.7) | 1 (2.0) | |
| Number of cycles received prior to ICI-M | 3.0 (2.0, 6.0) | 2.0 (1.0, 4.0) | 0.029 |
| Time to initial ICI-M/d | 71.0 (43.0, 169.0) | 47.0 (27.0, 90.0) | 0.006 |
| CTCAE grade of initial ICI-M/n(%) | 0.864 | ||
| Grade 1 | 162 (92.0) | 45 (90.0) | |
| Grade 2 | 14 (8.0) | 5 (10.0) | |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 160.0) | 85.0 (40.0, 260.0) | 0.683 |
| Peak CK-MB/(ng·mL-1) | 2.8 (1.8, 5.9) | 4.8 (2.4, 9.1) | 0.019 |
| Hospitalization/n(%) | 21 (11.9) | 7 (14.0) | 0.882 |
| Systemic steroids use/n(%) | 10 (5.7) | 6 (12.0) | 0.221 |
| Temporary ICI discontinuation/n(%) | 41 (23.3) | 12 (24.0) | 1.000 |
表2 ICI-M复发或新发其他类型irAEs的危险因素探索
Tab 2 Risk factors associated with recurrent ICI-M or new-onset irAEs
| Variable | No recurrent ICI-M/new irAEs (n=176) | Recurrent ICI-M/new irAEs (n=50) | P value |
|---|---|---|---|
| Age/year | 67.0 (61.0, 71.0) | 67.0 (62.0, 73.0) | 0.535 |
| Male/n(%) | 157 (89.2) | 44 (88.0) | 1.000 |
| BMI/(kg·m-2) | 22.9 ± 3.4 | 22.5 ± 3.3 | 0.483 |
| Coronary artery disease/n(%) | 28 (15.9) | 11 (22.0) | 0.427 |
| Hyperlipidemia/n(%) | 9 (5.1) | 5 (10.0) | 0.351 |
| Hypertension/n(%) | 63 (35.8) | 18 (36.0) | 1.000 |
| Diabetes/n(%) | 23 (13.1) | 6 (12.0) | 1.000 |
| Chronic kidney disease/n(%) | 2 (1.1) | 3 (6.0) | 0.129 |
| Histology/n(%) | 0.788 | ||
| Squamous cell carcinoma | 64 (36.4) | 17 (34.0) | |
| Adenocarcinoma | 69 (39.2) | 23 (46.0) | |
| Other NSCLC | 22 (12.5) | 6 (12.0) | |
| SCLC | 21 (11.9) | 4 (8.0) | |
| Disease stage/n(%) | 0.146 | ||
| Stage Ⅱ‒Ⅲ | 59 (33.5) | 23 (46.0) | |
| Stage Ⅳ | 117 (66.5) | 27 (54.0) | |
| ECOG performance status①/n(%) | 0.459 | ||
| 0 | 20 (14.8) | 4 (9.3) | |
| 1 | 113 (83.7) | 39 (90.7) | |
| 2 | 2 (1.5) | 0 (0) | |
| Hemoglobin/(g·L-1) | 130.0 (116.0, 140.5) | 128.5 (118.0, 142.0) | 0.951 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 0.366 |
| HbA1c/% | 5.8 (5.5, 6.3) | 5.8 (5.7, 6.3) | 0.384 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.9 (86.3, 101.3) | 94.1 (81.6, 101.2) | 0.655 |
| Radiotherapy/n(%) | 58 (33.0) | 16 (32.0) | 1.000 |
| ICI type after initial ICI-M/n(%) | 1.000 | ||
| PD-1 monotherapy | 150 (85.2) | 43 (86.0) | |
| PD-L1 monotherapy | 26 (14.8) | 7 (14.0) | |
| Anti-tumor treatment after initial ICI-M/n(%) | 0.244 | ||
| ICIs monotherapy | 45 (25.6) | 15 (30.0) | |
| Combination with chemotherapy | 109 (61.9) | 27 (54.0) | |
| Combination with targeted therapy | 12 (6.8) | 7 (14.0) | |
| Combination with chemotherapy and targeted therapy | 10 (5.7) | 1 (2.0) | |
| Number of cycles received prior to ICI-M | 3.0 (2.0, 6.0) | 2.0 (1.0, 4.0) | 0.029 |
| Time to initial ICI-M/d | 71.0 (43.0, 169.0) | 47.0 (27.0, 90.0) | 0.006 |
| CTCAE grade of initial ICI-M/n(%) | 0.864 | ||
| Grade 1 | 162 (92.0) | 45 (90.0) | |
| Grade 2 | 14 (8.0) | 5 (10.0) | |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 160.0) | 85.0 (40.0, 260.0) | 0.683 |
| Peak CK-MB/(ng·mL-1) | 2.8 (1.8, 5.9) | 4.8 (2.4, 9.1) | 0.019 |
| Hospitalization/n(%) | 21 (11.9) | 7 (14.0) | 0.882 |
| Systemic steroids use/n(%) | 10 (5.7) | 6 (12.0) | 0.221 |
| Temporary ICI discontinuation/n(%) | 41 (23.3) | 12 (24.0) | 1.000 |
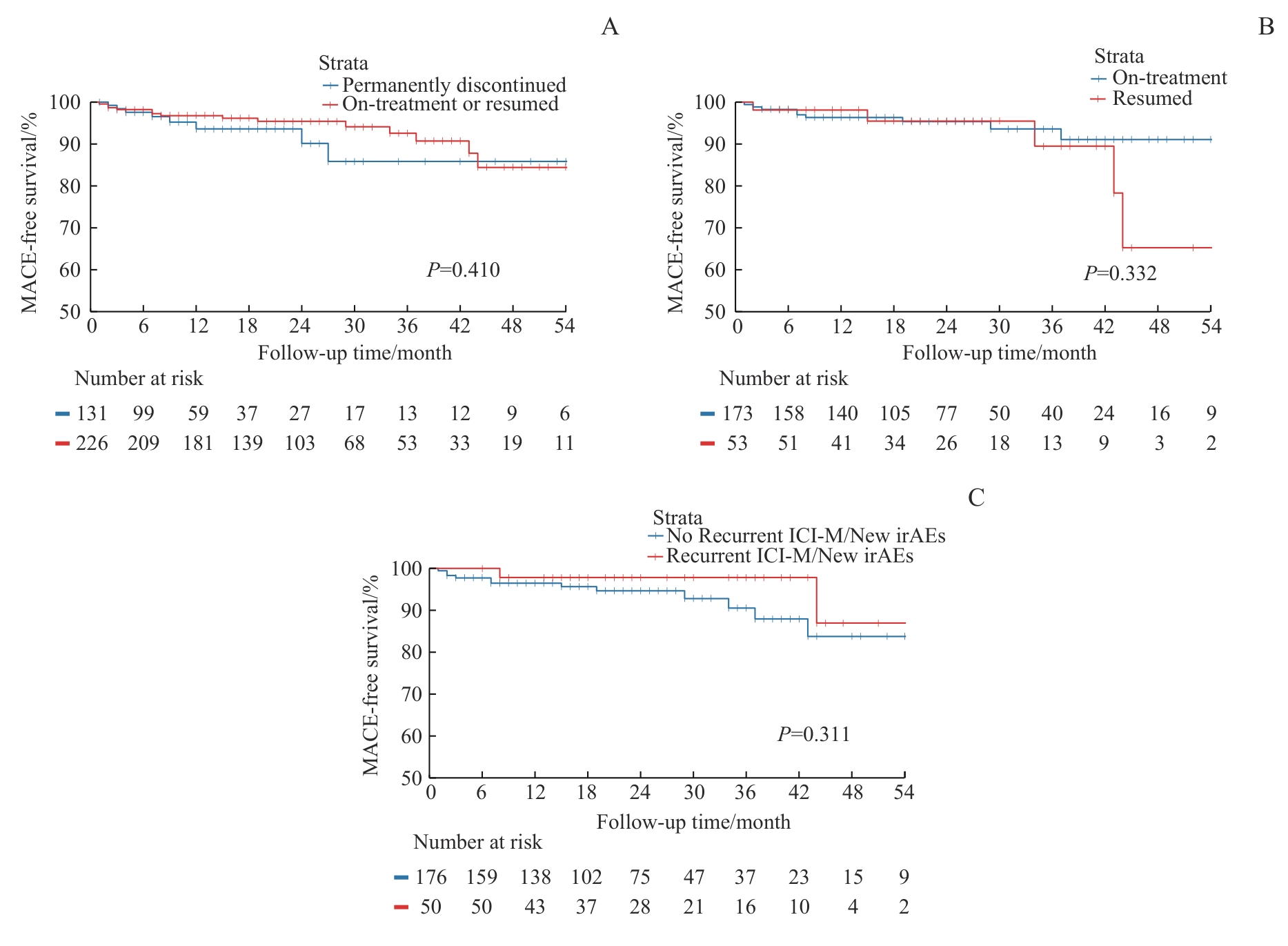
图3 MACE发生风险的Kaplan-Meier曲线Note: A. Kaplan-Meier curves for MACE between the permanently discontinued group and the on-treatment or resumed group. B. Kaplan-Meier curves for MACE between the on-treatment and the resumed group. C. Kaplan-Meier curves for MACE between patients with and without recurrent ICI-M or new-onset irAEs.
Fig 3 Kaplan-Meier curves for MACE incidence
| Factor | Multivariable analysis | |
|---|---|---|
| HR (95%CI) | P value | |
| On-treatment or resumed ICIs | 0.75 (0.28‒1.98) | 0.556 |
| Coronary artery disease | 2.53 (1.04‒6.17) | 0.041 |
| CTCAE grade of initial ICI-M | ||
| Grade 1 | Ref | |
| Grade 2 | 5.26 (1.91‒14.46) | 0.001 |
| Systemic steroids use for initial ICI-M | 0.63 (0.18‒2.18) | 0.469 |
| ECOG performance status | ||
| 0 | Ref | |
| 1 | 1.62 (0.20‒13.20) | 0.652 |
| 2 | 1.45 (0.06‒32.45) | 0.815 |
| Number of cycles received prior to ICI-M | 1.03 (0.97‒1.09) | 0.359 |
| Ongoing anti-tumor treatment | ||
| ICIs monotherapy | Ref | |
| Combination with chemotherapy | 0.70 (0.25‒1.95) | 0.500 |
| Combination with targeted therapy | 2.38 (0.56‒10.20) | 0.243 |
| Combination with chemotherapy and targeted therapy | 0.65 (0.07‒5.98) | 0.700 |
表3 ICI-M患者MACE事件的多因素Cox回归分析
Tab 3 Multivariable Cox regression analysis of factors associated with MACE in patients with ICI-M
| Factor | Multivariable analysis | |
|---|---|---|
| HR (95%CI) | P value | |
| On-treatment or resumed ICIs | 0.75 (0.28‒1.98) | 0.556 |
| Coronary artery disease | 2.53 (1.04‒6.17) | 0.041 |
| CTCAE grade of initial ICI-M | ||
| Grade 1 | Ref | |
| Grade 2 | 5.26 (1.91‒14.46) | 0.001 |
| Systemic steroids use for initial ICI-M | 0.63 (0.18‒2.18) | 0.469 |
| ECOG performance status | ||
| 0 | Ref | |
| 1 | 1.62 (0.20‒13.20) | 0.652 |
| 2 | 1.45 (0.06‒32.45) | 0.815 |
| Number of cycles received prior to ICI-M | 1.03 (0.97‒1.09) | 0.359 |
| Ongoing anti-tumor treatment | ||
| ICIs monotherapy | Ref | |
| Combination with chemotherapy | 0.70 (0.25‒1.95) | 0.500 |
| Combination with targeted therapy | 2.38 (0.56‒10.20) | 0.243 |
| Combination with chemotherapy and targeted therapy | 0.65 (0.07‒5.98) | 0.700 |
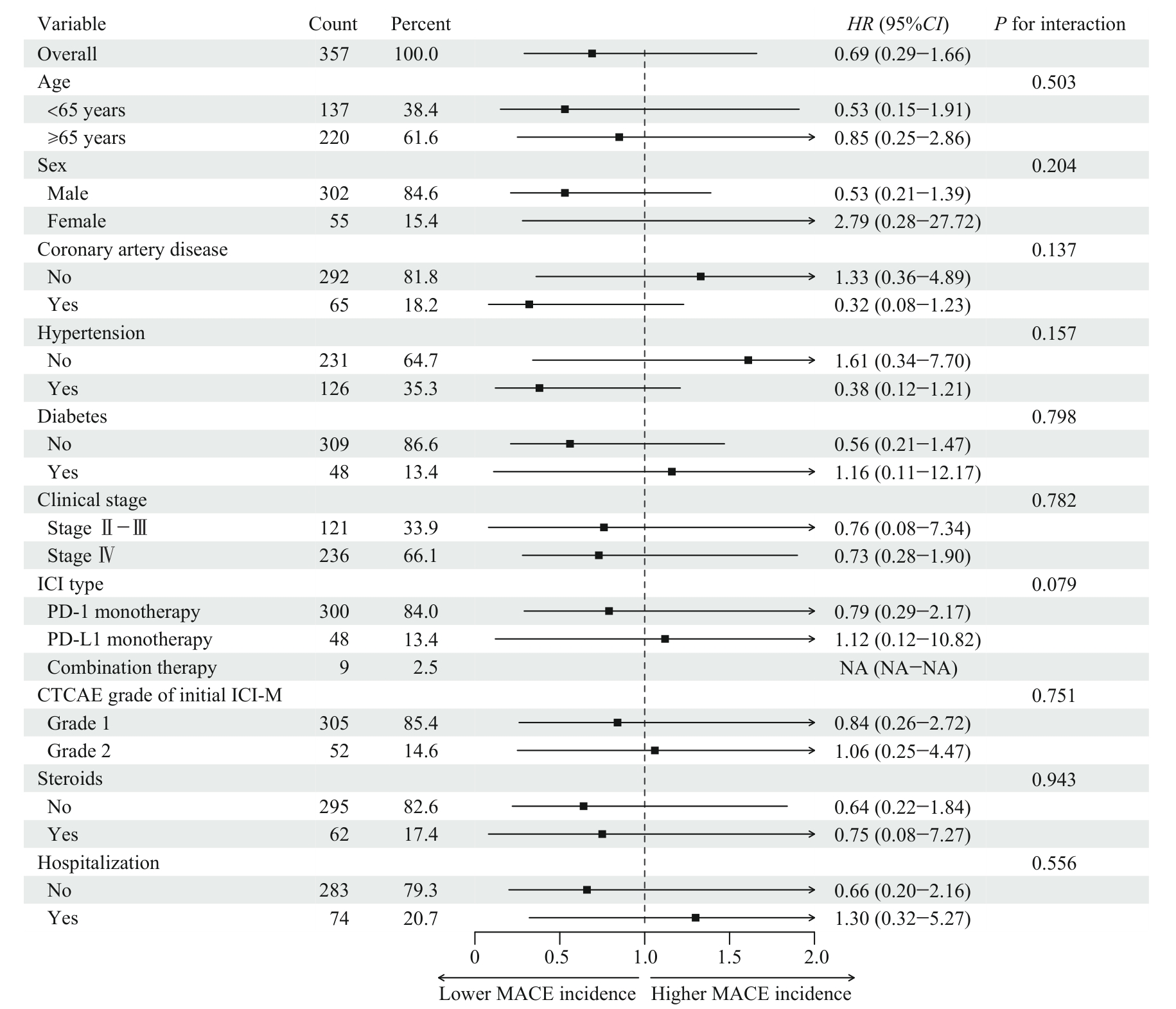
图4 未停药或ICIs重启免疫治疗对MACE事件影响的亚组分析Note: If there were fewer than 10 events in a subgroup, the analysis was not performed. NA—not applicable.
Fig 4 Subgroup analysis of the effect of on-treatment or resumption of ICIs therapy on MACE
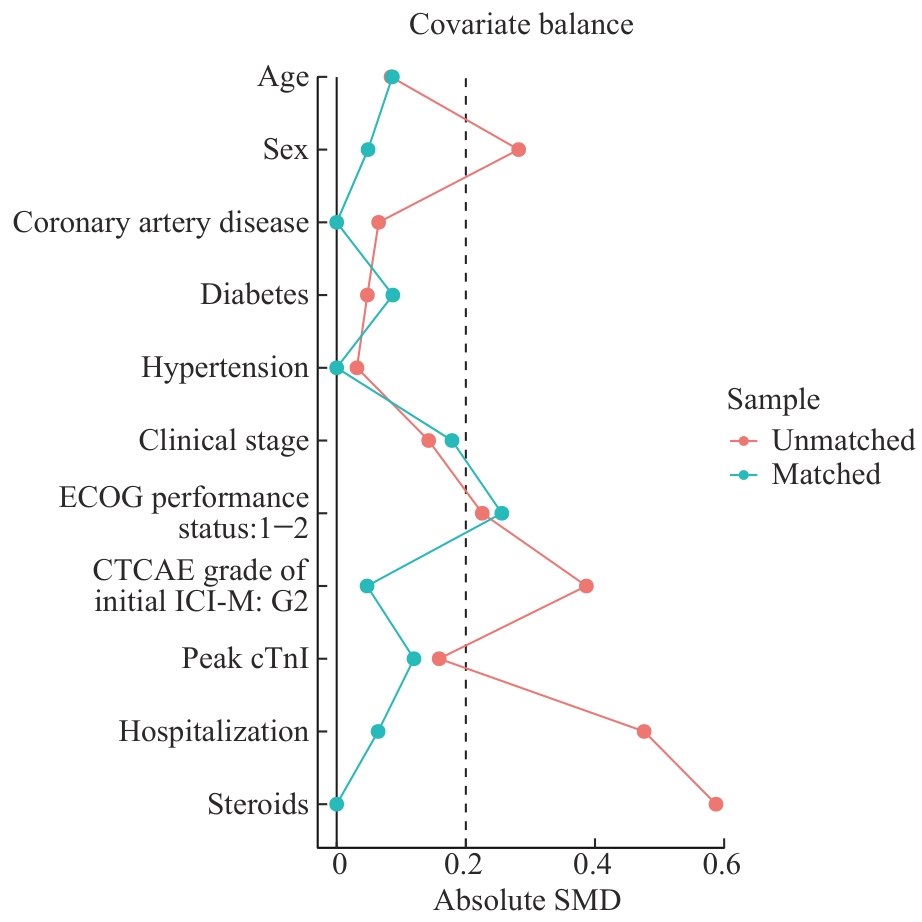
图5 倾向性评分匹配前后协变量SMD值变化
Fig 5 Comparison of SMDs before and after propensity score matching
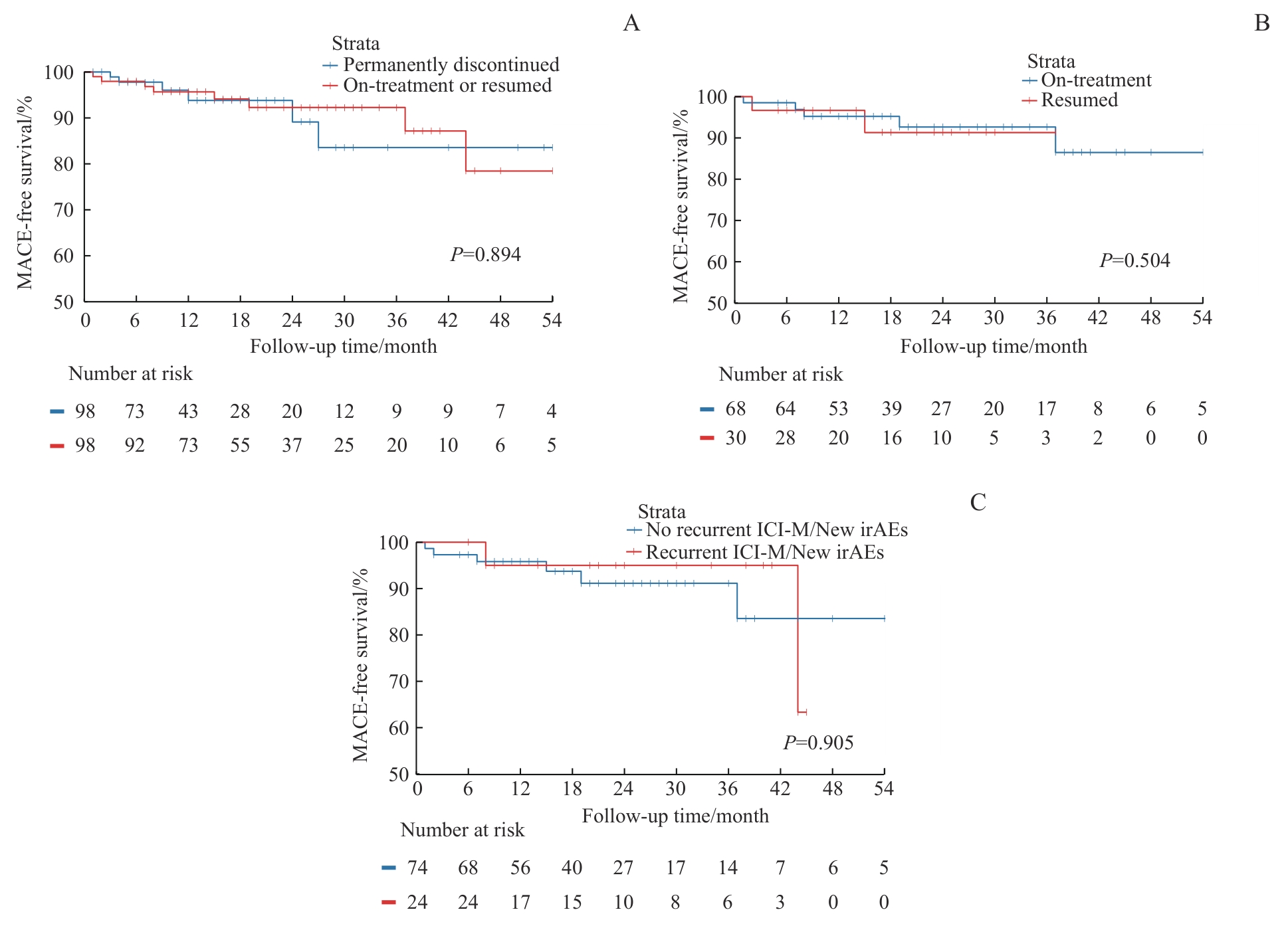
图6 倾向性评分匹配后MACE发生风险的Kaplan-Meier曲线Note: A. Kaplan-Meier curves for MACE between the permanently discontinued group and the on-treatment or resumed group. B. Kaplan-Meier curves for MACE between the on-treatment and the resumed group. C. Kaplan-Meier curves for MACE between patients with and without recurrent ICI-M or new-onset irAEs.
Fig 6 Kaplan-Meier curves for MACE after propensity score matching
| [1] | Ribas A, Wolchok J D. Cancer immunotherapy using checkpoint blockade[J]. Science, 2018, 359(6382): 1350-1355. |
| [2] | Schneider B J, Ismaila N, Aerts J, et al. Lung cancer surveillance after definitive curative-intent therapy: ASCO guideline[J]. J Clin Oncol, 2020, 38(7): 753-766. |
| [3] | Schonfeld S J, Tucker M A, Engels E A, et al. Immune-related adverse events after immune checkpoint inhibitors for melanoma among older adults[J]. JAMA Netw Open, 2022, 5(3): e223461. |
| [4] | Wang D Y, Salem J E, Cohen J V, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis[J]. JAMA Oncol, 2018, 4(12): 1721-1728. |
| [5] | Mahmood S S, Fradley M G, Cohen J V, et al. Myocarditis in patients treated with immune checkpoint inhibitors[J]. J Am Coll Cardiol, 2018, 71(16): 1755-1764. |
| [6] | Salem J E, Manouchehri A, Moey M, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study[J]. Lancet Oncol, 2018, 19(12): 1579-1589. |
| [7] | Vasbinder A, Chen Y, Procureur A, et al. Biomarker trends, incidence, and outcomes of immune checkpoint inhibitor-induced myocarditis[J]. JACC CardioOncol, 2022, 4(5): 689-700. |
| [8] | Curigliano G, Lenihan D, Fradley M, et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations[J]. Ann Oncol, 2020, 31(2): 171-190. |
| [9] | Schneider B J, Naidoo J, Santomasso B D, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update[J]. J Clin Oncol, 2021, 39(36): 4073-4126. |
| [10] | 中国抗癌协会整合肿瘤心脏病学分会, 中华医学会心血管病学分会肿瘤心脏病学学组, 中国医师协会心血管内科医师分会肿瘤心脏病学专业委员会, 等. 免疫检查点抑制剂相关心肌炎监测与管理中国专家共识(2020版)[J]. 中国肿瘤临床, 2020, 47(20): 1027-1038. |
| Society of Integrative Cardio-Oncology China Anti-Cancer Association, The Cardio-Oncology Group of the Chinese Society of Cardiovascular Diseases of Chinese Medical Association, Chinese College of Cardiovascular Physicians Specialized Committee on Cardio-Oncology Chinese Medical Docotor Association, et al. Chinese expert consensus on the surveillance and management of immune checkpoint inhibitor-related myocarditis (2020 version)[J]. Chinese Journal of Clinical Oncology, 2020, 47(20): 1027-1038. | |
| [11] | Herrmann J, Lenihan D, Armenian S, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement[J]. Eur Heart J, 2022, 43(4): 280-299. |
| [12] | Zannad F, Cannon C P, Cushman W C, et al. Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: a multicentre, randomised, double-blind trial[J]. Lancet, 2015, 385(9982): 2067-2076. |
| [13] | Dziura J D, Post L A, Zhao Q, et al. Strategies for dealing with missing data in clinical trials: from design to analysis[J]. Yale J Biol Med, 2013, 86(3): 343-358. |
| [14] | Austin P C. Some methods of propensity-score matching had superior performance to others: results of an empirical investigation and Monte Carlo simulations[J]. Biom J, 2009, 51(1): 171-184. |
| [15] | Coustal C, Vanoverschelde J, Quantin X, et al. Prognosis of immune checkpoint inhibitors-induced myocarditis: a case series[J]. J Immunother Cancer, 2023, 11(5): e004792. |
| [16] | Dolladille C, Ederhy S, Sassier M, et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events in patients with cancer[J]. JAMA Oncol, 2020, 6(6): 865-871. |
| [17] | L'Orphelin J M, da Silva A, Cabon J, et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events: a retrospective study from VigiBase update in 2024 looking for emergent safety signals[J]. BMJ Open, 2024, 14(12): e091708. |
| [18] | Pollack M H, Betof A, Dearden H, et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma[J]. Ann Oncol, 2018, 29(1): 250-255. |
| [19] | Simonaggio A, Michot J M, Voisin A L, et al. Evaluation of readministration of immune checkpoint inhibitors after immune-related adverse events in patients with cancer[J]. JAMA Oncol, 2019, 5(9): 1310-1317. |
| [20] | Santini F C, Rizvi H, Plodkowski A J, et al. Safety and efficacy of re-treating with immunotherapy after immune-related adverse events in patients with NSCLC[J]. Cancer Immunol Res, 2018, 6(9): 1093-1099. |
| [21] | Mulholland M, Chalou A, Andersson S H A, et al. Progenitor exhausted PD-1+ T cells are cellular targets of immune checkpoint inhibition in atherosclerosis[J]. Nat Cardiovasc Res, 2025, 4(10): 1311-1328. |
| [22] | Barcia Durán J G, Das D, Gildea M, et al. Immune checkpoint landscape of human atherosclerosis and influence of cardiometabolic factors[J]. Nat Cardiovasc Res, 2024, 3(12): 1482-1502. |
| [23] | van Dorst D C H, Uyl T J J, van der Veldt A A M, et al. Onset and progression of atherosclerosis in patients with melanoma treated with immune checkpoint inhibitors[J]. J Immunother Cancer, 2025, 13(4): e011226. |
| [24] | Drobni Z D, Gongora C, Taron J, et al. Impact of immune checkpoint inhibitors on atherosclerosis progression in patients with lung cancer[J]. J Immunother Cancer, 2023, 11(7): e007307. |
| [25] | Drobni Z D, Alvi R M, Taron J, et al. Association between immune checkpoint inhibitors with cardiovascular events and atherosclerotic plaque[J]. Circulation, 2020, 142(24): 2299-2311. |
| [26] | Guo M N, VanderWalde A M, Yu X H, et al. Immune checkpoint inhibitor rechallenge safety and efficacy in stage Ⅳ non-small cell lung cancer patients after immune-related adverse events[J]. Clin Lung Cancer, 2022, 23(8): 686-693. |
| [27] | Chen X, Jiang A M, Zhang R, et al. Immune checkpoint inhibitor-associated cardiotoxicity in solid tumors: real-world incidence, risk factors, and prognostic analysis[J]. Front Cardiovasc Med, 2022, 9: 882167. |
| [28] | Lee D H, Armanious M, Huang J, et al. Case of pembrolizumab-induced myocarditis presenting as torsades de pointes with safe re-challenge[J]. J Oncol Pharm Pract, 2020, 26(6): 1544-1548. |
| [29] | Eslinger C, Walden D, Barry T, et al. Rechallenge with switching immune checkpoint inhibitors following autoimmune myocarditis in a patient with lynch syndrome[J]. J Natl Compr Cancer Netw, 2023, 21(9): 894-899. |
| [30] | Shalata W, Attal Z G, Shhadi R, et al. Tolerated re-challenge of immunotherapy in a patient with ICI associated myocarditis: a case report and literature review[J]. Medicina (Kaunas), 2023, 59(11): 1946. |
| [1] | 杜鑫, 李雪冰, 李永伟. 巨噬细胞代谢重编程在复发性流产中的作用综述[J]. 上海交通大学学报(医学版), 2026, 46(4): 537-544. |
| [2] | 李广慧, 冯晓玲. 复发性流产中胎盘细胞铁死亡的研究进展[J]. 上海交通大学学报(医学版), 2025, 45(10): 1383-1389. |
| [3] | 杜芳, 周凌云, 陈姣, 刘丹波, 向泓先, 陈海飞. 复发难治性多发性骨髓瘤伴多病灶髓外浸润合并肺腺癌1例报道[J]. 上海交通大学学报(医学版), 2025, 45(1): 122-128. |
| [4] | 崔芷嫣, 陈尧, 陶悦, 沈树红, 李慧. PRPS1 I72位点突变对急性淋巴细胞白血病耐药性的影响及其机制研究[J]. 上海交通大学学报(医学版), 2023, 43(8): 977-987. |
| [5] | 黄华艳, 徐张闻笛, 夏立亮, 虞永峰, 陆舜. 表皮生长因子受体突变型晚期非小细胞肺癌免疫治疗的研究进展[J]. 上海交通大学学报(医学版), 2023, 43(5): 611-618. |
| [6] | 涂娟娟, 金志明. 免疫检查点抑制剂治疗转移性结直肠癌的研究进展[J]. 上海交通大学学报(医学版), 2023, 43(2): 250-255. |
| [7] | 吴雷, 夏一梦. PetCO2监测型鼻咽通气道在阻塞型睡眠呼吸暂停综合征患者胃镜精查麻醉中的应用研究[J]. 上海交通大学学报(医学版), 2023, 43(12): 1542-1547. |
| [8] | 韩婷, 吕纯鑫, 卓萌, 夏青, 刘腾飞, 吴秀奇, 林晓琳, 肖秀英. 进展期胃癌免疫治疗不良反应的相关因素及预后分析[J]. 上海交通大学学报(医学版), 2022, 42(8): 1053-1061. |
| [9] | 金磊, 徐文彬, 叶晨静, 阎骅. 泊沙康唑对血液恶性肿瘤化疗患者的预防性抗真菌作用[J]. 上海交通大学学报(医学版), 2022, 42(6): 792-796. |
| [10] | 郑诗凡, 马皎. 肿瘤干细胞代谢在肿瘤发展中作用的研究进展[J]. 上海交通大学学报(医学版), 2022, 42(6): 825-832. |
| [11] | 朱田雨, 宗春燕, 许诗琼, 葛盛芳, 范先群, 贾仁兵. 结膜黑色素瘤组织病理学特征、Ki-67表达和预后的关系[J]. 上海交通大学学报(医学版), 2022, 42(5): 617-623. |
| [12] | 邓露, 李佳怡. 点阵CO2激光治疗女性压力性尿失禁的研究进展[J]. 上海交通大学学报(医学版), 2022, 42(5): 685-689. |
| [13] | 王学宏, 陈旭卓, 毛懿, 沈达, 张善勇. 青少年不同发育阶段颞下颌关节盘锚固术后复发率的差异[J]. 上海交通大学学报(医学版), 2022, 42(2): 173-177. |
| [14] | 林艳艳, 许岩, 李慧. 儿童急性淋巴细胞白血病化学治疗常规药物耐药机制的研究进展[J]. 上海交通大学学报(医学版), 2022, 42(2): 211-217. |
| [15] | 胡宁宁, 张丹, 邹军, 张翀, 林芙君, 蒋更如. 单用他克莫司治疗特发性膜性肾病的效果及安全性评估[J]. 上海交通大学学报(医学版), 2022, 42(12): 1685-1692. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||