上海交通大学学报(医学版) ›› 2022, Vol. 42 ›› Issue (12): 1712-1719.doi: 10.3969/j.issn.1674-8115.2022.12.009
魏逸凡( ), 朱月钮, 孔祥莓, 许雅雅, 朱晓东()
), 朱月钮, 孔祥莓, 许雅雅, 朱晓东()
收稿日期:2022-07-15
接受日期:2022-12-15
出版日期:2022-12-28
发布日期:2022-12-28
通讯作者:
朱晓东,E-mail:xinhuaxiaodong@126.com。作者简介:魏逸凡(1994—),女,住院医师,硕士生;电子信箱:weiyifan1994s@163.com。
WEI Yifan(), ZHU Yueniu, KONG Xiangmei, XU Yaya, ZHU Xiaodong()
Received:2022-07-15
Accepted:2022-12-15
Online:2022-12-28
Published:2022-12-28
Contact:
ZHU Xiaodong,E-mail:xinhuaxiaodong@126.com.摘要:
目的·探讨同步间歇指令通气(synchronized intermittent mandatory ventilation,SIMV)模式下机械通气早期小儿膈肌的形态与功能变化状况。方法·纳入2020年10月—2021年12月收治于上海交通大学医学院附属新华医院小儿急危重症医学科(Pediatric Intensive Care Unit,PICU)并接受机械通气治疗满96 h的患儿,通过床旁超声连续测量膈肌的相关数据,分析接受机械通气治疗后3个不同时间点(0、48、96 h)膈肌相关变化。各时间点间皮下脂肪厚度、皮下脂肪萎缩率、膈肌厚度、膈肌移动度比较均采用Kruskal-Wallis H检验,其中膈肌厚度进一步采用Bonferroni法校正显著性水平进行事后两两比较;各时间点膈肌收缩速度、膈肌增厚率、膈肌萎缩率比较均采用单因素方差分析。结果·纳入46例测量数据完整的患儿,平均年龄2.94(1.35,7.00)岁,男女各23例。导致需要机械通气治疗的主要病因为肺炎(52.17%);观察期间呼吸机的参数选择与机体氧合状态亦无明显差异(均P>0.05)。机械通气早期(96 h内)有50%的患儿出现腹部皮下脂肪的萎缩,36.96%患儿营养供给出现障碍(禁食与肠外营养支持),93.5%患儿接受糖皮质激素治疗,但3个时间点间腹部皮下脂肪的萎缩程度差异无统计学意义(均P>0.05)。床旁超声检测3个时间点的双侧膈肌厚度均发生明显萎缩(均P=0.000);机械通气48 h后右侧膈肌萎缩率为4.27%±7.36%,左侧膈肌萎缩率为3.88%±6.85%;机械通气96 h后右侧膈肌萎缩率为7.69%±7.74%,左侧膈肌萎缩率为7.55%±7.69%;双侧膈肌的萎缩率在机械通气最初的48 h内比48~96 h内更高(P=0.000)。3个时间点膈肌的功能相关指标(膈肌移动度、膈肌收缩速率、膈肌增厚率)比较,差异均无统计学意义。结论·床旁膈肌超声可以用来监测机械通气儿童的膈肌萎缩程度。SIMV模式的机械通气早期(96 h内)可引起小儿膈肌的结构性萎缩,且以最初48 h更为显著。膈肌早期形态学变化尚未影响患儿膈肌功能。
中图分类号:
魏逸凡, 朱月钮, 孔祥莓, 许雅雅, 朱晓东. 早期机械通气对小儿膈肌形态与功能的影响[J]. 上海交通大学学报(医学版), 2022, 42(12): 1712-1719.
WEI Yifan, ZHU Yueniu, KONG Xiangmei, XU Yaya, ZHU Xiaodong. Effects of early mechanical ventilation on the morphology and function of the diaphragm in children[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(12): 1712-1719.
| Indicator | M(Q1, Q3)/n(%) |
|---|---|
| General data | |
| Age/year | 2.94 (1.35, 7.00) |
| Male/female/n(%) | 23 (50.00)/23 (50.00) |
| Height/cm | 97.50 (78.00, 115.00) |
| Weight/kg | 13.08 (10.00, 22.00) |
| BMI/(kg·m-2) | 15.94 (13.55, 17.85) |
| Baseline abdominal fat thickness/mm | 0.70 (0.57, 0.89) |
| Abdominal fat atrophy/n(%) | 23 (50.00) |
| Body surface area/m2 | 0.60 (0.43, 0.87) |
| Clinical score system | |
| PCIS | 88.00 (79.00, 94.00) |
| PRISM Ⅲ | 6.00 (3.00, 10.00) |
| Primary disease | |
| Respiratory diseases/n(%) | 10 (21.74) |
| Neurological diseases/n(%) | 20 (43.48) |
| Hematologic diseases/n(%) | 4 (8.70) |
| Digestive diseases/n(%) | 5 (10.87) |
| Musculoskeletal diseases/n(%) | 1 (2.17) |
| Urinary diseases/n(%) | 1 (2.17) |
| Endocrine diseases/n(%) | 5 (10.87) |
| Etiology | |
| Pneumonia/n(%) | 24 (52.17) |
| CNS lesions/n(%) | 16 (34.78) |
| Septic pyemia/n(%) | 6 (13.04) |
| Complication | |
| MODS/n(%) | 6 (13.04) |
| Treatment | |
| Glucocorticoid/n(%) | 43 (93.50) |
| Parenteral nutrition/n(%) | 7 (15.22) |
| Fasting/n(%) | 10 (21.74) |
| Surgical interventions/n(%) | 26 (56.52) |
| Prognosis | |
| Weaning failure/n(%) | 18 (39.13) |
| Mortality in PICU/n(%) | 10 (21.74) |
| Duration of mechanical ventilation/d | 8.00 (7.00, 12.00) |
| Hospitalization days in PICU/d | 20.00 (11.00, 31.00) |
表1 46例患儿的基本资料
Tab 1 Main clinical characteristics of 46 children
| Indicator | M(Q1, Q3)/n(%) |
|---|---|
| General data | |
| Age/year | 2.94 (1.35, 7.00) |
| Male/female/n(%) | 23 (50.00)/23 (50.00) |
| Height/cm | 97.50 (78.00, 115.00) |
| Weight/kg | 13.08 (10.00, 22.00) |
| BMI/(kg·m-2) | 15.94 (13.55, 17.85) |
| Baseline abdominal fat thickness/mm | 0.70 (0.57, 0.89) |
| Abdominal fat atrophy/n(%) | 23 (50.00) |
| Body surface area/m2 | 0.60 (0.43, 0.87) |
| Clinical score system | |
| PCIS | 88.00 (79.00, 94.00) |
| PRISM Ⅲ | 6.00 (3.00, 10.00) |
| Primary disease | |
| Respiratory diseases/n(%) | 10 (21.74) |
| Neurological diseases/n(%) | 20 (43.48) |
| Hematologic diseases/n(%) | 4 (8.70) |
| Digestive diseases/n(%) | 5 (10.87) |
| Musculoskeletal diseases/n(%) | 1 (2.17) |
| Urinary diseases/n(%) | 1 (2.17) |
| Endocrine diseases/n(%) | 5 (10.87) |
| Etiology | |
| Pneumonia/n(%) | 24 (52.17) |
| CNS lesions/n(%) | 16 (34.78) |
| Septic pyemia/n(%) | 6 (13.04) |
| Complication | |
| MODS/n(%) | 6 (13.04) |
| Treatment | |
| Glucocorticoid/n(%) | 43 (93.50) |
| Parenteral nutrition/n(%) | 7 (15.22) |
| Fasting/n(%) | 10 (21.74) |
| Surgical interventions/n(%) | 26 (56.52) |
| Prognosis | |
| Weaning failure/n(%) | 18 (39.13) |
| Mortality in PICU/n(%) | 10 (21.74) |
| Duration of mechanical ventilation/d | 8.00 (7.00, 12.00) |
| Hospitalization days in PICU/d | 20.00 (11.00, 31.00) |
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Oxygenation status | |||||
| SaO2/% | 97.80 (95.2, 99.40) | 97.00 (91.63, 99.23) | 97.50 (89.80, 99.23) | 0.73 | 0.70 |
| OI/mmHg | 349.55±166.03 | 305.97±159.04 | 321.24±161.00 | 0.90 | 0.41 |
| PaCO2/mmHg | 42.32±8.60 | 44.44±10.85 | 43.23±8.37 | 0.60 | 0.55 |
| Ventilator parameter | |||||
| Ppeak/cmH2O | 17.61±4.43 | 16.72±4.04 | 16.04±3.83 | 1.46 | 0.24 |
| Pmean/cmH2O | 8.83±3.48 | 8.26±3.28 | 7.49±2.60 | 1.78 | 0.17 |
| PEEP/cmH2O | 4.57±1.91 | 4.46±1.72 | 4.04±1.45 | 0.89 | 0.42 |
| FiO2/% | 36.76±11.43 | 35.07±10.63 | 34.40±10.12 | 0.39 | 0.68 |
| MVe/(L·min-1) | 3.38±1.83 | 3.21±1.64 | 3.03±1.48 | 0.42 | 0.66 |
| TV/(mL·kg-1) | 7.54±3.31 | 7.44±2.89 | 7.04±2.85 | 2.50 | 0.09 |
表2 PICU患儿机械通气后多个时间点的机体氧合状态及呼吸机参数设定比较
Tab 2 Comparison of the oxygenation status of children in PICU and the ventilator parameter settings at multiple time points after mechanical ventilation
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Oxygenation status | |||||
| SaO2/% | 97.80 (95.2, 99.40) | 97.00 (91.63, 99.23) | 97.50 (89.80, 99.23) | 0.73 | 0.70 |
| OI/mmHg | 349.55±166.03 | 305.97±159.04 | 321.24±161.00 | 0.90 | 0.41 |
| PaCO2/mmHg | 42.32±8.60 | 44.44±10.85 | 43.23±8.37 | 0.60 | 0.55 |
| Ventilator parameter | |||||
| Ppeak/cmH2O | 17.61±4.43 | 16.72±4.04 | 16.04±3.83 | 1.46 | 0.24 |
| Pmean/cmH2O | 8.83±3.48 | 8.26±3.28 | 7.49±2.60 | 1.78 | 0.17 |
| PEEP/cmH2O | 4.57±1.91 | 4.46±1.72 | 4.04±1.45 | 0.89 | 0.42 |
| FiO2/% | 36.76±11.43 | 35.07±10.63 | 34.40±10.12 | 0.39 | 0.68 |
| MVe/(L·min-1) | 3.38±1.83 | 3.21±1.64 | 3.03±1.48 | 0.42 | 0.66 |
| TV/(mL·kg-1) | 7.54±3.31 | 7.44±2.89 | 7.04±2.85 | 2.50 | 0.09 |
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Thickness /cm | 0.69 (0.56, 0.90) | 0.74 (0.57, 0.89) | 0.70 (0.56, 0.91) | 1.06 | 0.59 |
| Atrophy rate /% | 0 (0, 0) | -1.30 (-8.80, 5.77) | 0 (-6.92, 7.81) | 1.06 | 0.59 |
表3 PICU患儿机械通气96 h期间的腹部皮下脂肪比较
Tab 3 Comparison of the abdominal subcutaneous fat of children in PICU during 96 h of mechanical ventilation
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Thickness /cm | 0.69 (0.56, 0.90) | 0.74 (0.57, 0.89) | 0.70 (0.56, 0.91) | 1.06 | 0.59 |
| Atrophy rate /% | 0 (0, 0) | -1.30 (-8.80, 5.77) | 0 (-6.92, 7.81) | 1.06 | 0.59 |
| Indicator | Position | MV | H value | P value | ||
|---|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | ||||
| Diaphragmatic thickness/mm | R-I | 2.82±0.73 | 2.68±0.70 | 2.57±0.65 | 38.68 | 0.000 |
| R-E | 2.47±0.66 | 2.36±0.64 | 2.26±0.58 | 43.92 | 0.000 | |
| L-I | 2.58±0.71 | 2.46±0.70 | 2.35±0.67 | 37.19 | 0.000 | |
| L-E | 2.25±0.62 | 2.16±0.60 | 2.08±0.59 | 44.38 | 0.000 | |
| DE/mm | R | 6.20 (4.09, 8.60) | 5.85 (3.79, 7.72) | 6.09 (4.96, 7.89) | 2.48 | 0.290 |
| L | 5.60 (3.95, 7.25) | 6.15 (4.23, 9.40) | 5.75 (4.10, 8.86) | 4.19 | 0.120 | |
| DCV/(mm·s-1) | R | 6.59±3.61 | 5.35±2.83 | 6.79±4.09 | 4.74 | 0.090 |
| L | 6.28±3.73 | 6.16±3.43 | 6.42±3.49 | 1.65 | 0.440 | |
| DTF/% | R | 14.28±4.98 | 13.85±5.52 | 13.43±5.02 | 0.54 | 0.760 |
| L | 14.75±5.70 | 13.64±4.44 | 13.37±4.77 | 0.84 | 0.660 | |
| DAR/% | R | ‒ | 4.27±7.36 | 7.69±7.74 | 43.92 | 0.000 |
| L | ‒ | 3.88±6.85 | 7.55±7.69 | 37.19 | 0.000 | |
表4 PICU患儿机械通气早期的膈肌床旁超声数据比较
Tab 4 Comparison of the diaphragmatic bedside ultrasound data of children in PICU during early-stage mechanical ventilation
| Indicator | Position | MV | H value | P value | ||
|---|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | ||||
| Diaphragmatic thickness/mm | R-I | 2.82±0.73 | 2.68±0.70 | 2.57±0.65 | 38.68 | 0.000 |
| R-E | 2.47±0.66 | 2.36±0.64 | 2.26±0.58 | 43.92 | 0.000 | |
| L-I | 2.58±0.71 | 2.46±0.70 | 2.35±0.67 | 37.19 | 0.000 | |
| L-E | 2.25±0.62 | 2.16±0.60 | 2.08±0.59 | 44.38 | 0.000 | |
| DE/mm | R | 6.20 (4.09, 8.60) | 5.85 (3.79, 7.72) | 6.09 (4.96, 7.89) | 2.48 | 0.290 |
| L | 5.60 (3.95, 7.25) | 6.15 (4.23, 9.40) | 5.75 (4.10, 8.86) | 4.19 | 0.120 | |
| DCV/(mm·s-1) | R | 6.59±3.61 | 5.35±2.83 | 6.79±4.09 | 4.74 | 0.090 |
| L | 6.28±3.73 | 6.16±3.43 | 6.42±3.49 | 1.65 | 0.440 | |
| DTF/% | R | 14.28±4.98 | 13.85±5.52 | 13.43±5.02 | 0.54 | 0.760 |
| L | 14.75±5.70 | 13.64±4.44 | 13.37±4.77 | 0.84 | 0.660 | |
| DAR/% | R | ‒ | 4.27±7.36 | 7.69±7.74 | 43.92 | 0.000 |
| L | ‒ | 3.88±6.85 | 7.55±7.69 | 37.19 | 0.000 | |
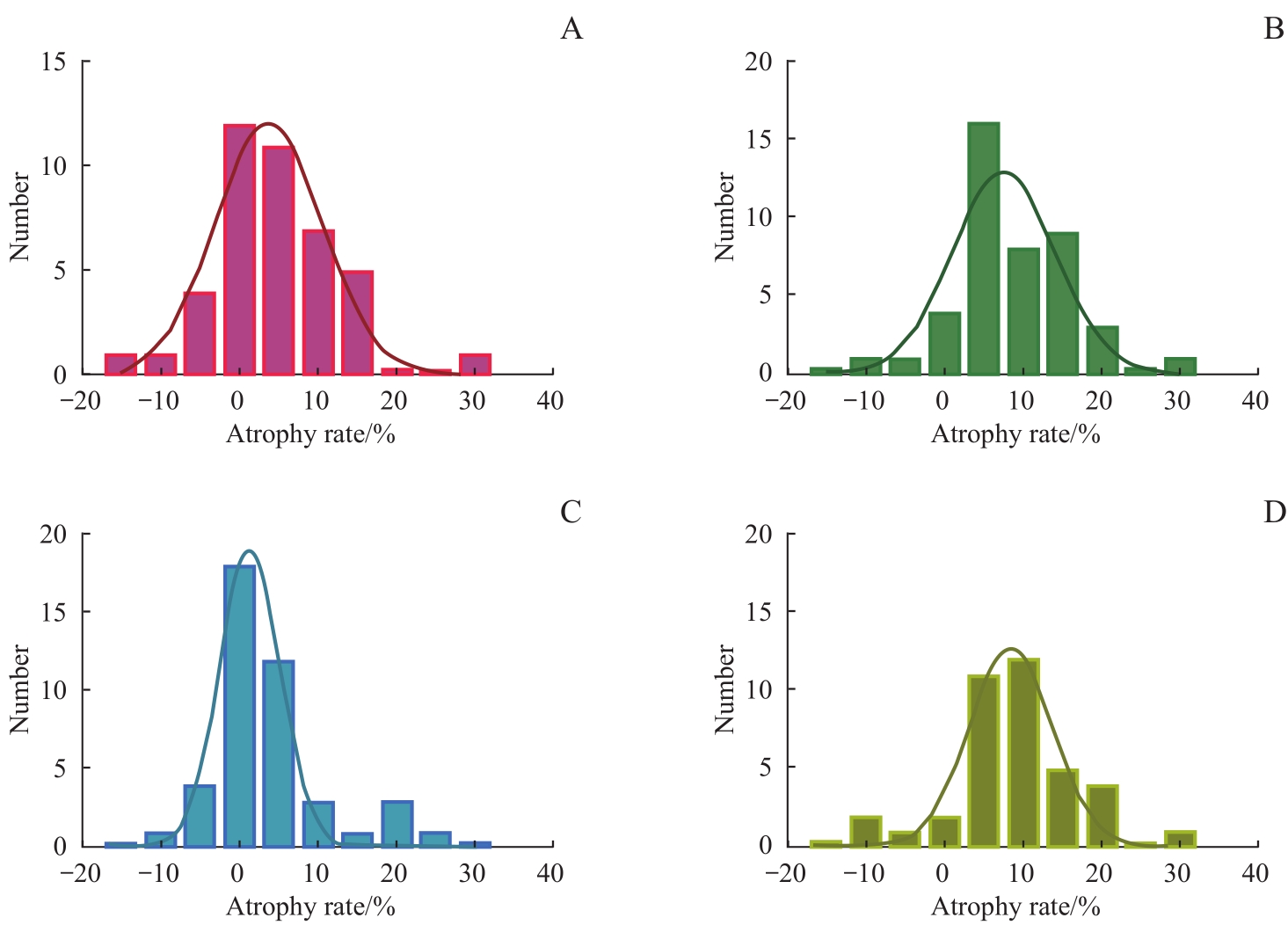
图1 机械通气48 h、96 h后膈肌萎缩率频数分布Note: A. Frequency distribution of atrophy rate of right diaphragm after 48 h of mechanical ventilation. B. Frequency distribution of atrophy rate of right diaphragm after 96 h of mechanical ventilation. C. Frequency distribution of atrophy rate of left diaphragm after 48 h of mechanical ventilation.D. Frequency distribution of atrophy rate of left diaphragm after 96 h of mechanical ventilation.
Fig1 Distribution of diaphragm atrophy rate after 48 h and 96 h of mechanical ventilation
| 1 | TOBIN M J, LAGHI F, JUBRAN A. Narrative review: ventilator-induced respiratory muscle weakness[J]. Ann Intern Med, 2010, 153(4): 240-245. |
| 2 | DE JONGHE B, BASTUJI-GARIN S, DURAND M C, et al. Respiratory weakness is associated with limb weakness and delayed weaning in critical illness[J]. Crit Care Med, 2007, 35(9): 2007-2015. |
| 3 | DEMOULE A, MOLINARI N, JUNG B, et al. Patterns of diaphragm function in critically ill patients receiving prolonged mechanical ventilation: a prospective longitudinal study[J]. Ann Inten Care, 2016, 6(1): 75. |
| 4 | BÉDUNEAU G, PHAM T, SCHORTGEN F, et al. Epidemiology of weaning outcome according to a new definition. the WIND study[J]. Am J Respir Crit Care Med, 2017, 195(6): 772-783. |
| 5 | DRES M, DUBÉ B P, MAYAUX J, et al. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients[J]. Am J Respir Crit Care Med, 2017, 195(1): 57-66. |
| 6 | KIM W Y, SUH H J, HONG S B, et al. Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation[J]. Crit Care Med, 2011, 39(12): 2627-2630. |
| 7 | GOLIGHER E C, DRES M, FAN E, et al. Mechanical ventilation-induced diaphragm atrophy strongly impacts clinical outcomes[J]. Am J Respir Crit Care Med, 2018, 197(2): 204-213. |
| 8 | DAMUTH E, MITCHELL J A, BARTOCK J L, et al. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: a systematic review and meta-analysis[J]. Lancet Respir Med, 2015, 3(7): 544-553. |
| 9 | GROSU H B, LEE Y I, LEE J, et al. Diaphragm muscle thinning in patients who are mechanically ventilated[J]. Chest, 2012, 142(6): 1455-1460. |
| 10 | LEVINE S, NGUYEN T, TAYLOR N, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans[J]. N Engl J Med, 2008, 358(13): 1327-1335. |
| 11 | POWERS S K, SHANELY R A, COOMBES J S, et al. Mechanical ventilation results in progressive contractile dysfunction in the diaphragm[J]. J Appl Physiol (1985), 2002, 92(5): 1851-1858. |
| 12 | JABER S, PETROF B J, JUNG B, et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans[J]. Am J Respir Crit Care Med, 2011, 183(3): 364-371. |
| 13 | SHANELY R A, ZERGEROGLU M A, LENNON SL, et al. Mechanical ventilation-induced diaphragmatic atrophy is associated with oxidative injury and increased proteolytic activity[J]. Am J Respir Crit Care Med, 2002, 166(10): 1369-1374. |
| 14 | GOLIGHER E C, FAN E, HERRIDGE M S, et al. Evolution of diaphragm thickness during mechanical ventilation. impact of inspiratory effort[J]. Am J Respir Crit Care Med, 2015, 192(9): 1080-1088. |
| 15 | OROZCO-LEVI M, LLORETA J, MINGUELLA J, et al. Injury of the human diaphragm associated with exertion and chronic obstructive pulmonary disease[J]. Am J Respir Crit Care Med, 2001, 164(9): 1734-1739. |
| 16 | GOLIGHER E C, LAGHI F, DETSKY M E, et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity[J]. Intensive Care Med, 2015, 41(4): 642-649. |
| 17 | FAYSSOIL A, BEHIN A, OGNA A, et al. Diaphragm: pathophysiology and ultrasound imaging in neuromuscular disorders[J]. J Neuromuscul Dis, 2018, 5(1): 1-10. |
| 18 | FARIAS J A, FRUTOS F, ESTEBAN A, et al. What is the daily practice of mechanical ventilation in pediatric intensive care units? A multicenter study[J]. Intensive Care Med, 2004, 30(5): 918-925. |
| 19 | TAKAZAKURA R, TAKAHASHI M, NITTA N, et al. Diaphragmatic motion in the sitting and supine positions: healthy subject study using a vertically open magnetic resonance system[J]. J Magn Reson Imaging, 2004, 19(5): 605-609. |
| 20 | YAMAGUTI W P, PAULIN E, SHIBAO S, et al. Ultrasound evaluation of diaphragmatic mobility in different postures in healthy subjects[J]. J Bras Pneumol, 2007, 33(4): 407-413. |
| 21 | VIVIER E, MEKONTSO DESSAP A, DIMASSI S, et al. Diaphragm ultrasonography to estimate the work of breathing during non-invasive ventilation[J]. Intensive Care Med, 2012, 38(5): 796-803. |
| 22 | MATAMIS D, SOILEMEZI E, TSAGOURIAS M, et al. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications[J]. Intensive Care Med, 2013, 39(5): 801-810. |
| 23 | MCCOOL F D, CONOMOS P, BENDITT J O, et al. Maximal inspiratory pressures and dimensions of the diaphragm[J]. Am J Respir Crit Care Med, 1997, 155(4): 1329-1334. |
| 24 | COHN D, BENDITT J O, EVELOFF S, et al. Diaphragm thickening during inspiration[J]. J Appl Physiol (1985), 1997, 83(1): 291-296. |
| 25 | LIU Y Y, LI L F. Ventilator-induced diaphragm dysfunction in critical illness[J]. Exp Biol Med (Maywood), 2018, 243(17/18): 1329-1337. |
| 26 | POWERS S K, WIGGS M P, SOLLANEK K J, et al. Ventilator-induced diaphragm dysfunction: cause and effect[J]. Am J Physiol Regul Integr Comp Physiol, 2013, 305(5): R464-R477. |
| 27 | POWERS S K, KAVAZIS A N, LEVINE S. Prolonged mechanical ventilation alters diaphragmatic structure and function[J]. Crit Care Med, 2009, 37(10 Suppl): S347-S353. |
| 28 | SCHEPENS T, VERBRUGGHE W, DAMS K, et al. The course of diaphragm atrophy in ventilated patients assessed with ultrasound: a longitudinal cohort study[J]. Crit Care, 2015, 19: 422. |
| 29 | IJLAND M M, LEMSON J, VAN DER HOEVEN J G, et al. The impact of critical illness on the expiratory muscles and the diaphragm assessed by ultrasound in mechanical ventilated children[J]. Ann Intensive Care, 2020, 10(1): 115. |
| 30 | GLAU C L, CONLON T W, HIMEBAUCH A S, et al. Progressive diaphragm atrophy in pediatric acute respiratory failure[J]. Pediatr Crit Care Med, 2018, 19(5): 406-411. |
| 31 | JOHNSON R W, NG K W P, DIETZ A R, et al. Muscle atrophy in mechanically-ventilated critically ill children[J]. PLoS One, 2018, 13(12): e0207720. |
| 32 | LEE E P, HSIA S H, HSIAO H F, et al. Evaluation of diaphragmatic function in mechanically ventilated children: an ultrasound study[J]. PLoS One, 2017, 12(8): e0183560. |
| 33 | GRASSI A, FERLICCA D, LUPIERI E, et al. Assisted mechanical ventilation promotes recovery of diaphragmatic thickness in critically ill patients: a prospective observational study[J]. Crit Care, 2020, 24: 85. |
| 34 | ZAMBON M, BECCARIA P, MATSUNO J, et al. Mechanical ventilation and diaphragmatic atrophy in critically ill patients: an ultrasound study[J]. Crit Care Med, 2016, 44(7): 1347-1352. |
| 35 | POWERS S K, DECRAMER M, GAYAN-RAMIREZ G, et al. Pressure support ventilation attenuates ventilator-induced protein modifications in the diaphragm[J]. Crit Care, 2008, 12(6): 191. |
| 36 | DEVOTO G, GALLO F, MARCHELLO C, et al. Prealbumin serum concentrations as a useful tool in the assessment of malnutrition in hospitalized patients[J]. Clin Chem, 2006, 52(12): 2281-2285. |
| 37 | JIANG J R. Ultrasonographic evaluation of liver/spleen movements and extubation outcome[J]. Chest, 2004, 126(1): 179-185. |
| 38 | SUMMERHILL E M, EL-SAMEED Y A, GLIDDEN T J, et al. Monitoring recovery from diaphragm paralysis with ultrasound[J]. Chest, 2008, 133(3): 737-743. |
| 39 | DININO E, GARTMAN E J, SETHI J M, et al. Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation[J]. Thorax, 2014, 69(5): 423-427. |
| 40 | FARGHALY S, HASAN A A. Diaphragm ultrasound as a new method to predict extubation outcome in mechanically ventilated patients[J]. Aust Crit Care, 2017, 30(1): 37-43. |
| 41 | GOTTESMAN E, MCCOOL F D. Ultrasound evaluation of the paralyzed diaphragm[J]. Am J Respir Crit Care Med, 1997, 155(5): 1570-1574. |
| 42 | ZAMBON M, GRECO M, BOCCHINO S, et al. Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: a systematic review[J]. Intensive Care Med, 2017, 43(1): 29-38. |
| 43 | NEWTH C J L, VENKATARAMAN S, WILLSON D F, et al. Weaning and extubation readiness in pediatric patients[J]. Pediatr Crit Care Med, 2009, 10(1): 1-11. |
| 44 | DOORDUIN J, VAN HEES H W H, VAN DER HOEVEN J G, et al. Monitoring of the respiratory muscles in the critically ill[J]. Am J Respir Crit Care Med, 2013, 187(1): 20-27. |
| 45 | CATTAPAN S E, LAGHI F, TOBIN M J. Can diaphragmatic contractility be assessed by airway twitch pressure in mechanically ventilated patients? [J]. Thorax, 2003, 58(1): 58-62. |
| [1] | 王少雁, 李超, 黄硕, 吴书其, 陈素芸. 不同年龄段儿童与青少年18F-FDG PET/CT显像肝脏本底与纵隔血池生理分布特征及影响因素分析[J]. 上海交通大学学报(医学版), 2026, 46(4): 496-501. |
| [2] | 徐州琳, 尹高生, 李沅聪, 杨云恒, 郑琦, 杨萍. 天麻素调控自噬在心肌梗死后骨骼肌萎缩中的作用研究[J]. 上海交通大学学报(医学版), 2026, 46(3): 301-311. |
| [3] | 阿布力克木·阿木提, 李悠然, 杨晨蝶, GuanPoh Tay, 冯硕, 张瑞岩, 王晓群. 基于血管内超声分析载脂蛋白B控制水平对冠状动脉斑块进展影响的队列研究[J]. 上海交通大学学报(医学版), 2026, 46(3): 312-321. |
| [4] | 曹轶磊, 刘维纯, 张晓欣, 赵爱民. 低剂量阿司匹林对遗传性易栓症患者子宫血流灌注的改善作用[J]. 上海交通大学学报(医学版), 2026, 46(2): 200-205. |
| [5] | 程先茹, 曹煜雯, 田沃土, 曹立. 肌萎缩侧索硬化相关基因致痉挛性截瘫表型:临床、影像及遗传学分析[J]. 上海交通大学学报(医学版), 2026, 46(2): 256-264. |
| [6] | 万朋杰, 杨绍芳, 齐珺. 局部窄谱中波紫外线联合地奈德乳膏治疗儿童中重度特应性皮炎的疗效观察[J]. 上海交通大学学报(医学版), 2026, 46(1): 132-136. |
| [7] | 吴青青, 曹毅, 陆丽娜, 陶怡菁, 冯海霞, 颜伟慧, 王莹. 高剂量维生素D在儿童短肠综合征合并维生素D不足/缺乏中的应用[J]. 上海交通大学学报(医学版), 2026, 46(1): 54-59. |
| [8] | 刘美伶, 包磊, 闵令钊, 魏嘉, 华丽, 王晓强. 儿童四叠体池蛛网膜囊肿临床特点及疗效分析:一项定量回顾性研究[J]. 上海交通大学学报(医学版), 2026, 46(1): 66-74. |
| [9] | 超声引导儿童神经阻滞中国专家共识(2025版)编写组. 超声引导儿童神经阻滞中国专家共识(2025版)[J]. 上海交通大学学报(医学版), 2025, 45(9): 1079-1098. |
| [10] | 王治琪, 王莹. 儿童炎症性肠病相关贫血的诊治研究进展[J]. 上海交通大学学报(医学版), 2025, 45(9): 1232-1238. |
| [11] | 蒋婕, 张泓, 伦赫远, 潘芬, 于方圆, 何平. 儿童肺炎克雷伯菌感染分子流行病学特征[J]. 上海交通大学学报(医学版), 2025, 45(8): 1027-1034. |
| [12] | 梁书源, 叶宝英, 程蔚蔚. 超声指标和血液指标预测胎儿生长受限的研究现状[J]. 上海交通大学学报(医学版), 2025, 45(8): 1059-1065. |
| [13] | 何晨, 颜斯蕾, 周维涛, 凌勇, 于宁宁, 蒋鲲, 钱莉玲. 囊性纤维化合并变应性支气管肺曲菌病的临床分析及文献整合研究[J]. 上海交通大学学报(医学版), 2025, 45(8): 1066-1073. |
| [14] | 陆晔峰, 高磊青, 倪晓筱, 富晶晶. 儿童肝移植术后早期血糖及血脂的多时间点监测与影响因素分析[J]. 上海交通大学学报(医学版), 2025, 45(4): 443-451. |
| [15] | 刘田恬, 赵奕琳, 宁菁菁, 张育才, 王春霞. 儿童脓毒症预后相关长链非编码RNA筛选及竞争性内源RNA网络的构建[J]. 上海交通大学学报(医学版), 2025, 45(3): 282-291. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||